Department of Medical Oncology, Tata Memorial Centre, Mumbai, India; Homi Bhabha National Institute, Mumbai, India.
Homi Bhabha National Institute, Mumbai, India; Biostatistics, Tata Memorial Centre, Mumbai, India.
ESMO Open. 2022 Oct;7(5):100558. doi: 10.1016/j.esmoop.2022.100558. Epub 2022 Aug 22.
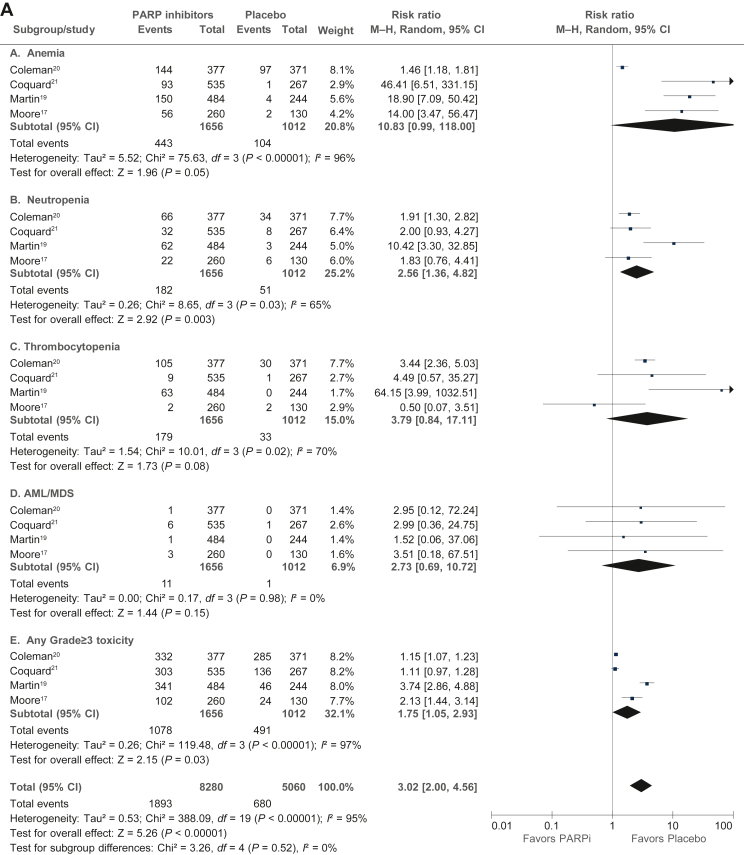
We synthesize the efficacy and toxicity of poly(ADP-ribose) polymerase inhibitors (PARPis) in patients with newly diagnosed advanced ovarian cancer.
We manually extracted individual patient data (IPD) for progression-free survival (PFS) from published survival curves of randomized controlled trials (RCTs) that compared PARPi versus placebo as maintenance therapy in first-line treatment, for whole study populations and subgroups, based on BRCA1/BRCA2 mutation (germline and/or somatic) and homologous recombination deficiency (HRD) status, using WebPlotDigitizer software. The respective PFS curves for each study and combined population were reconstructed from extracted IPD. The primary outcome was PFS in combined whole population and subgroups.
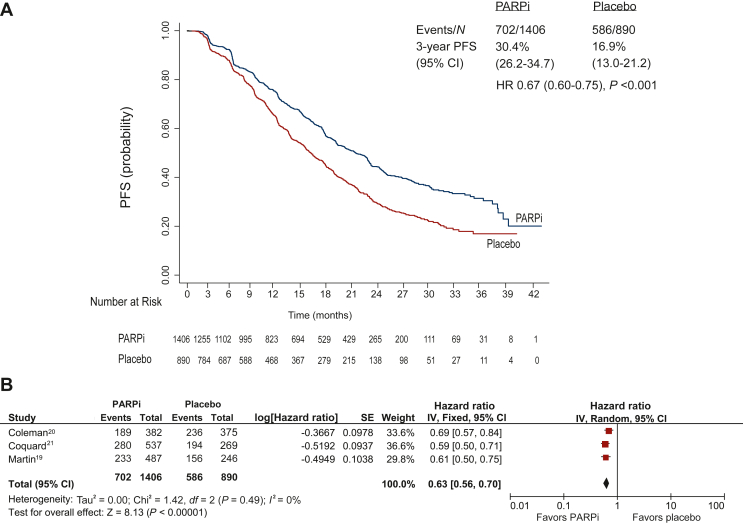
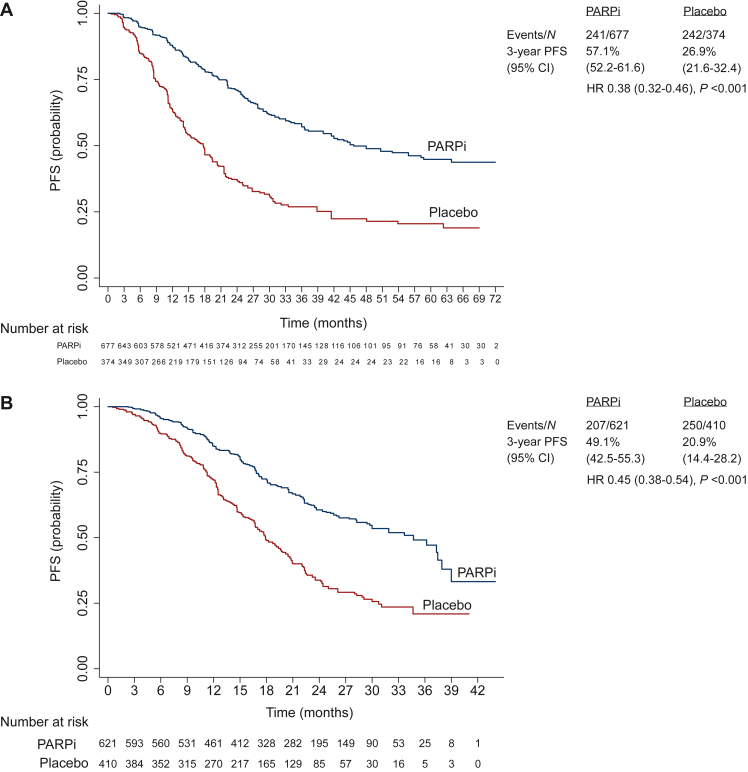
In IPD analysis of combined population from three RCTs, with 2296 patients and 1287 events, PFS was significantly longer in PARPi versus placebo [median 20.4 (95% confidence interval (CI) 18.6-21.9) versus 14.9 (95% CI 13.9-16.5) months, respectively; hazard ratio (HR) 0.67, 95% CI 0.60-0.75; P < 0.001]. In IPD subgroup analyses from four eligible RCTs (2687 patients and 1485 events), median PFS was significantly longer in PARPi versus placebo arm, in the BRCA-mutated (45.7 versus 17.7 months, respectively; HR 0.38, 95% CI 0.32-0.46; P < 0.001), HRD-positive including BRCA-mutated (34.7 versus 17.9 months, respectively; HR 0.45, 95% CI 0.38-0.54; P < 0.001), and HRD positive excluding BRCA-mutated (22.3 versus 13.1 months, respectively; HR 0.47, 95% CI 0.34-0.65; P < 0.001) subgroups, but not in the HRD-negative (15.0 versus 11.3 months, respectively; HR 0.90, 95% CI 0.76-1.05; P = 0.75) subgroup. Results of trial-level meta-analysis were concordant with IPD analysis in whole population and subgroups.
Among newly diagnosed ovarian cancer patients, PARPi maintenance therapy significantly improves PFS in those with germline and/or somatic BRCA mutation and/or HRD-positive tumor but not in those with HRD-negative tumor.
我们综合了聚(ADP-核糖)聚合酶抑制剂(PARPi)在新诊断的晚期卵巢癌患者中的疗效和毒性。
我们使用 WebPlotDigitizer 软件,从比较 PARPi 与安慰剂作为一线治疗维持治疗的随机对照试验(RCT)发表的生存曲线中手动提取无进展生存期(PFS)的个体患者数据(IPD)。对于整个研究人群和亚组,基于 BRCA1/BRCA2 突变(种系和/或体细胞)和同源重组缺陷(HRD)状态,基于 BRCA1/BRCA2 突变(种系和/或体细胞)和同源重组缺陷(HRD)状态,我们对整个研究人群和亚组进行了分析。使用 WebPlotDigitizer 软件,从比较 PARPi 与安慰剂作为一线治疗维持治疗的随机对照试验(RCT)发表的生存曲线中手动提取无进展生存期(PFS)的个体患者数据(IPD)。使用 WebPlotDigitizer 软件,从比较 PARPi 与安慰剂作为一线治疗维持治疗的随机对照试验(RCT)发表的生存曲线中手动提取无进展生存期(PFS)的个体患者数据(IPD)。使用 WebPlotDigitizer 软件,从比较 PARPi 与安慰剂作为一线治疗维持治疗的随机对照试验(RCT)发表的生存曲线中手动提取无进展生存期(PFS)的个体患者数据(IPD)。相应的每个研究和合并人群的 PFS 曲线都是从提取的 IPD 中重建的。主要结局是合并人群和亚组的 PFS。
在三项 RCT 的合并人群的 IPD 分析中,共有 2296 名患者和 1287 例事件,PARPi 与安慰剂相比,PFS 显著延长[中位数 20.4(95%置信区间(CI)18.6-21.9)与 14.9(95%CI 13.9-16.5)个月,分别;风险比(HR)0.67,95%CI 0.60-0.75;P <0.001]。在四项合格 RCT 的 IPD 亚组分析中(2687 名患者和 1485 例事件),PARPi 与安慰剂组相比,PFS 中位数显著延长,BRCA 突变亚组(45.7 与 17.7 个月,分别;HR 0.38,95%CI 0.32-0.46;P <0.001),HRD 阳性包括 BRCA 突变亚组(34.7 与 17.9 个月,分别;HR 0.45,95%CI 0.38-0.54;P <0.001),和 HRD 阳性排除 BRCA 突变亚组(22.3 与 13.1 个月,分别;HR 0.47,95%CI 0.34-0.65;P <0.001),但在 HRD 阴性亚组(15.0 与 11.3 个月,分别;HR 0.90,95%CI 0.76-1.05;P=0.75)中则不然。整个人群和亚组的试验水平荟萃分析结果与 IPD 分析一致。
在新诊断的卵巢癌患者中,PARPi 维持治疗显著改善了种系和/或体细胞 BRCA 突变和/或 HRD 阳性肿瘤患者的 PFS,但不能改善 HRD 阴性肿瘤患者的 PFS。