Cazzaniga Marina Elena, Capici Serena, Cordani Nicoletta, Cogliati Viola, Pepe Francesca Fulvia, Riva Francesca, Cerrito Maria Grazia
School of Medicine and Surgery, Milano-Bicocca University, 20900 Monza, Italy.
Phase 1 Research Centre, ASST Monza, 20900 Monza, Italy.
J Clin Med. 2022 Aug 12;11(16):4710. doi: 10.3390/jcm11164710.
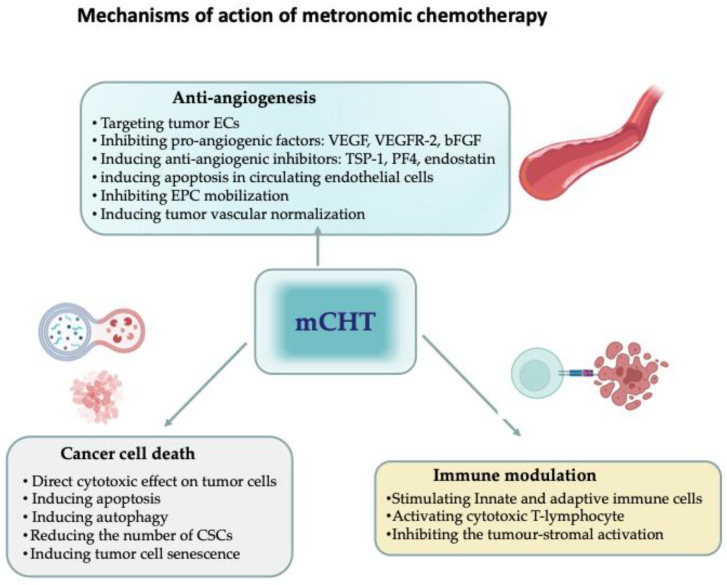
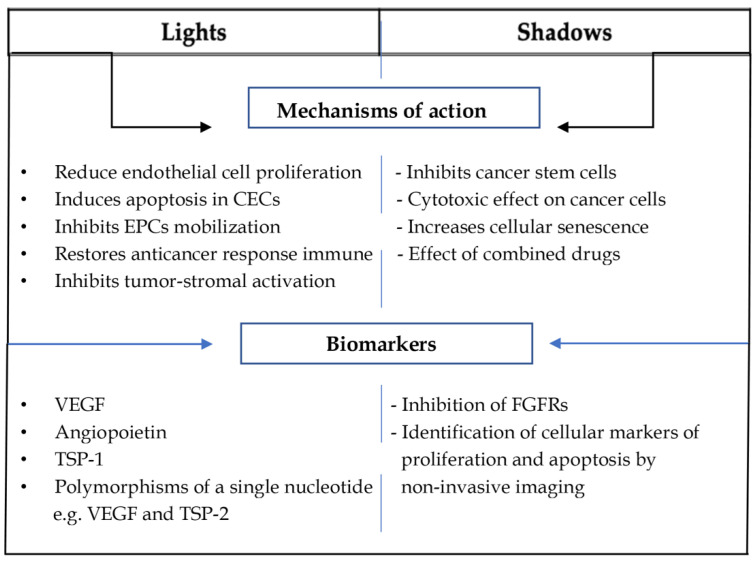
Metronomic chemotherapy (mCHT), defined as continuous administration of low-dose chemotherapeutic agents with no or short regular treatment-free intervals, was first introduced to the clinic in international guidelines in 2017, and, since then, has become one of the available strategies for the treatment of advanced breast cancer (ABC). Despite recent successes, many unsolved practical and theoretical issues remain to be addressed. The present review aims to identify the "lights and shadows" of mCHT in preclinical and clinical settings. In the preclinical setting, several findings indicate that one of the most noticeable effects of mCHT is on the tumor microenvironment, which, over the last twenty years, has been demonstrated to be pivotal in supporting tumor cell survival and proliferation. On the other hand, the direct effects on tumor cells have been less well-defined. In addition, critical items to be addressed are the lack of definition of an optimal biological dose (OBD), the method of administration of metronomic schedules, and the recognition and validation of predictive biomarkers. In the clinical context-where mCHT has mainly been used in a metastatic setting-low toxicity is the most well-recognised light of mCHT, whereas the type of study design, the absence of randomised trials and uncertainty in terms of doses and drugs remain among the shadows. In conclusion, growing evidence indicates that mCHT is a suitable treatment option for selected metastatic breast cancer (MBC) patients. Moreover, given its multimodal mechanisms of action, its addition to immunological and targeted therapies might represent a promising new approach to the treatment of MBC. More preclinical data are needed in this regard, which can only be obtained through support for translational research as the key link between basic science and patient care.
节拍化疗(mCHT)被定义为持续给予低剂量化疗药物,且无或有短时间的常规无治疗间隔期,于2017年首次被引入国际指南用于临床,自那时起,已成为晚期乳腺癌(ABC)的可用治疗策略之一。尽管近期取得了成功,但仍有许多未解决的实际和理论问题有待解决。本综述旨在确定mCHT在临床前和临床环境中的“亮点与阴影”。在临床前环境中,多项研究结果表明,mCHT最显著的作用之一是对肿瘤微环境的影响,在过去二十年中,已证明肿瘤微环境在支持肿瘤细胞存活和增殖方面起着关键作用。另一方面,对肿瘤细胞的直接作用尚不太明确。此外,需要解决的关键问题包括缺乏最佳生物学剂量(OBD)的定义、节拍给药方案的给药方法以及预测生物标志物的识别和验证。在临床环境中——mCHT主要用于转移性疾病——低毒性是mCHT最广为人知的亮点,而研究设计类型、缺乏随机试验以及剂量和药物方面的不确定性仍然是其阴影所在。总之,越来越多的证据表明,mCHT是选定的转移性乳腺癌(MBC)患者的合适治疗选择。此外,鉴于其多模式作用机制,将其添加到免疫治疗和靶向治疗中可能代表一种有前景的MBC治疗新方法。在这方面需要更多的临床前数据,而这只能通过支持转化研究来获得,转化研究是基础科学与患者护理之间的关键环节。