Scurto Lucia, Peluso Nicolò, Pascucci Federico, Sica Simona, De Nigris Francesca, Filipponi Marco, Minelli Fabrizio, Donati Tommaso, Tinelli Giovanni, Tshomba Yamume
Unit of Vascular Surgery, Fondazione Policlinico Universitario A. Gemelli I.R.C.C.S., Università Cattolica del Sacro Cuore, 00168 Roma, Italy.
Unit of Vascular Surgery, Fondazione Policlinico Universitario A. Gemelli I.R.C.C.S., 00168 Roma, Italy.
J Pers Med. 2022 Aug 4;12(8):1279. doi: 10.3390/jpm12081279.
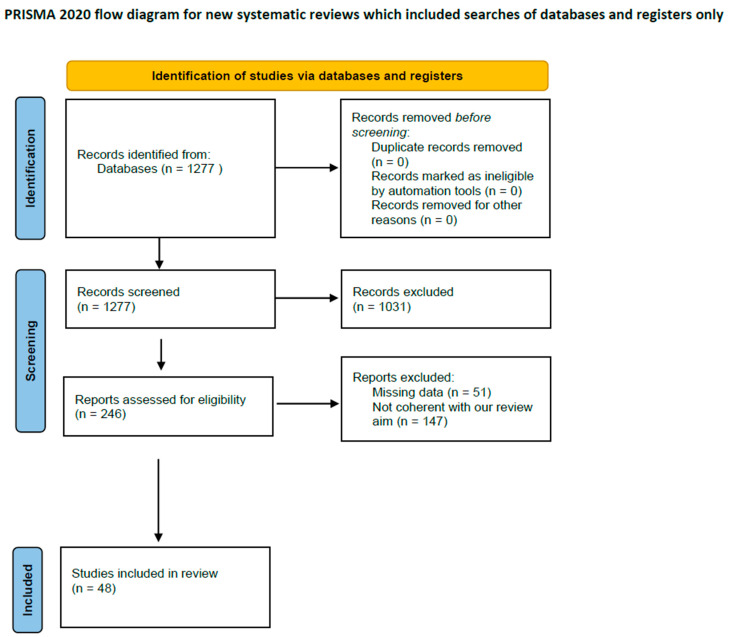
Aortic arch repair is a challenging intervention. Open surgical repair is still considered the gold standard, but in high-risk patients, it is not always a reasonable option, making endovascular approaches an enticing, when not the only available, alternative for treatment. The strategies more commonly adopted are surgical supra-aortic trunk (SAT) rerouting followed by deployment of a standard thoracic endoprosthesis, chimney techniques, custom-made scalloped, fenestrated, and branched devices, and in situ or physician-modified fenestrations. If we excluded techniques involving SAT rerouting where the arch anatomy is surgically modified in order to make deployment in the aortic arch of a standard thoracic endoprosthesis possible, in the other techniques, one or more SATs are incorporated in the thoracic endoprosthesis. In these cases, no matter what solution is adopted, because of the morphology of the aorta at this level, achieving an ideal sealing is extremely difficult, and endovascular treatments of the arch are burdened by an increased risk of type IA endoleaks. PubMed, EMBASE, and Cochrane Library were searched. We identified 1277 records. After reading titles, abstracts, and full texts, we excluded 1231 records. Exclusion criteria were low-quality evidence, abstracts, case reports, conference presentations, reviews, editorials, and expert opinions. A total of 48 studies were included, for a total of 3114 patients. A type IA endoleak occurred in 248 patients (7.7%) with a mean incidence of 18.8% in chimney procedures, 4.8% and 3%, respectively, in fenestrated and branched devices, and 2.2% in in situ fenestration. We excluded from our analysis scalloped technology that is used when the target vessel originates from a healthy landing zone and represents a different anatomical setting. Type IA endoleaks are a concern with all types of endovascular aortic arch repair, and they can compromise the outcomes of the procedure. The rate of type IA endoleaks appears to be significantly higher in chimney procedures. In order to maximize sealing, whenever possible, endovascular repair of the arch should be achieved with custom-made fenestrated devices. However, chimney configurations are still a valuable solution particularly in the emergency setting, although in such a procedure, to guarantee accurate postoperative management and follow-up, an imaging protocol could be useful.
主动脉弓修复是一项具有挑战性的干预措施。开放手术修复仍被视为金标准,但对于高危患者,它并不总是一个合理的选择,这使得血管内治疗方法成为一种诱人的(即使不是唯一可用的)治疗替代方案。更常用的策略包括手术重建主动脉弓上干(SAT),然后植入标准的胸段血管内假体、烟囱技术、定制的扇形、开窗和分支装置,以及原位或医生改良的开窗术。如果我们排除涉及SAT重建的技术(在这种技术中,主动脉弓解剖结构通过手术进行修改,以便能够在主动脉弓中植入标准的胸段血管内假体),在其他技术中,一个或多个SAT被纳入胸段血管内假体。在这些情况下,无论采用何种解决方案,由于该水平主动脉的形态,实现理想的密封极其困难,并且主动脉弓的血管内治疗存在IA型内漏风险增加的问题。我们检索了PubMed、EMBASE和Cochrane图书馆。我们识别出1277条记录。在阅读标题、摘要和全文后,我们排除了1231条记录。排除标准为低质量证据、摘要、病例报告、会议报告、综述、社论和专家意见。共纳入48项研究,涉及3114例患者。248例患者(7.7%)发生IA型内漏,烟囱技术的平均发生率为18.8%,开窗和分支装置分别为4.8%和3%,原位开窗为2.2%。我们在分析中排除了扇形技术,该技术用于目标血管起源于健康着陆区且代表不同解剖情况时。IA型内漏是所有类型的血管内主动脉弓修复都需要关注的问题,它们可能会影响手术结果。烟囱技术中IA型内漏的发生率似乎明显更高。为了最大限度地实现密封,只要有可能,主动脉弓的血管内修复应采用定制的开窗装置。然而,烟囱配置仍然是一种有价值的解决方案,特别是在紧急情况下,尽管在这样的手术中,为了保证准确的术后管理和随访,成像方案可能会有所帮助。