Fetal and Neonatal Institute, Division of Neonatology, Children's Hospital Los Angeles, Department of Pediatrics, Keck School of Medicine of the University of Southern California, Los Angeles, California.
Division of Pediatric Surgery, Children's Hospital Los Angeles, Los Angeles, CA Department of Surgery, Keck School of Medicine of the University of Southern California, Los Angeles, California.
J Surg Res. 2022 Dec;280:273-279. doi: 10.1016/j.jss.2022.07.022. Epub 2022 Aug 26.
Children with congenital heart disease (CHD) often experience feeding intolerance due to aspiration, inability to tolerate feed volume, or reflux within the first few months of life, requiring a surgically placed gastrostomy tube (GT) for durable enteral access. However, complications such as GT dislodgement, cellulitis, and leakage related to GT use are common. GT-related complications can lead to unscheduled pediatric surgery clinic or emergency room (ER) visits, which can be time consuming for the family and increase overall healthcare costs. We sought to identify factors associated with GT complications within 2 wk after GT surgery and 1-y after discharge home following GT placement in infants with CHD.
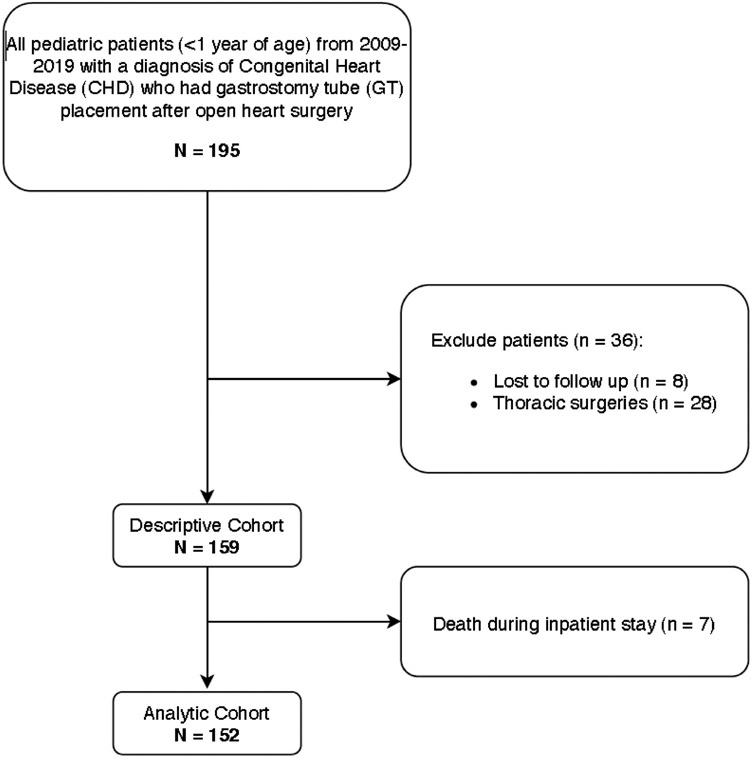
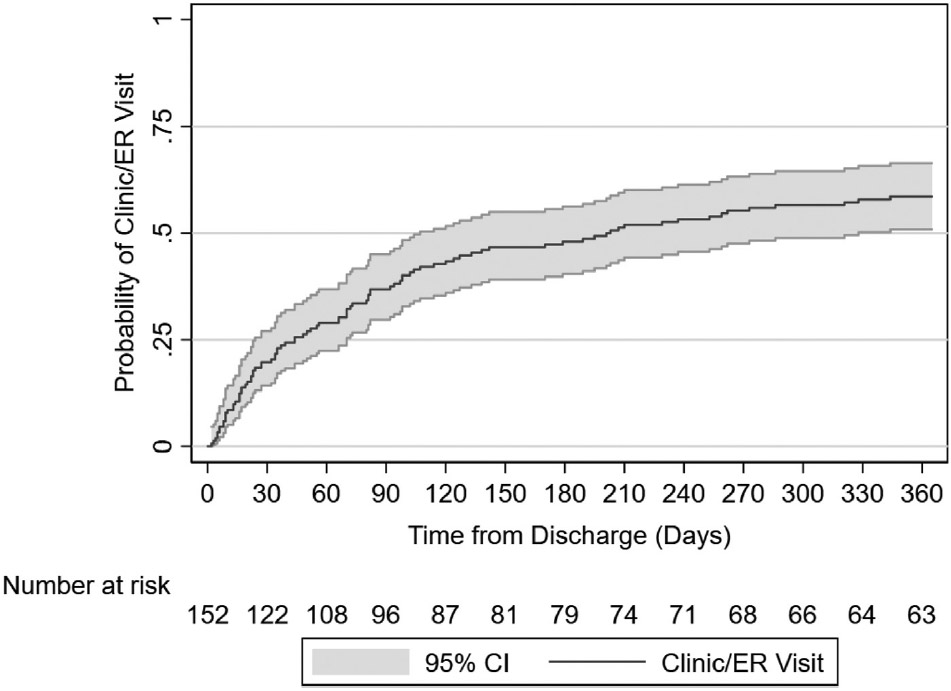
We performed a retrospective cohort study using the Society of Thoracic Surgeons database and electronic medical records from a tertiary children's hospital. We identified infants <1 y old underwent CHD surgery followed by GT surgery between September 2013-August 2018. Demographics, pre-operative feeding regimen, comorbidities, and GT-related utilization were measured. Postoperative GT complications (e.g., GT cellulitis, leakage, dislodgement, obstruction, and granulation tissue) within 2 wk after the GT surgery and an unplanned pediatric surgery clinic or ER visit within 1-y after discharge home were captured. Bivariate comparisons and multivariable logistic regression evaluated factors associated with GT complications and unplanned clinic or ER visits. A Kaplan-Meier failure curve examined the timing of ER/clinic visits.
Of 152 infants who underwent CHD then GT surgeries, 66% (N = 101) had postoperative GT complications. Overall, 83 unscheduled clinic visits were identified after discharge, with 37% (N = 31) due to concerns about granulation tissue. Of 137 ER visits, 48% (N = 66) were due to accidental GT dislodgement. Infants who were hospitalized for ≥2 wk after GT surgery had more complications than those discharged home within 2 wk of the GT surgery (40.6% versus 15.7%, P = 0.002). Infants receiving oral nutrition before CHD surgery (38.6% versus 60%, P=<0.001) or with single ventricle defects (19.8% versus 37.3%, P = 0.02) had fewer GT complications. After adjusting for type of cardiac anomaly, infants receiving oral nutrition prior to CHD surgery had a decreased likelihood of GT complications (odds ratio OR 0.46; 95% confidence intervals CI:0.23-0.93). A Kaplan-Meier failure curve demonstrated that 50% of the cohort experienced a complication leading to an unscheduled ER/clinic visit within 6 mo after discharge.
Unplanned visits to the ER or pediatric surgery clinic occur frequently for infants with CHD requiring a surgically placed GT. Oral feedings before cardiac surgery associated with fewer GT complications. Prolonged hospitalization associated with more GT complications. Optimizing outpatient care and family education regarding GT maintenance may reduce unscheduled visits for this high-risk, device-dependent infant population.
患有先天性心脏病 (CHD) 的儿童在生命的最初几个月中经常因吸入、不能耐受喂养量或反流而出现喂养不耐受,需要进行外科胃造口术 (GT) 以获得持久的肠内通路。然而,GT 移位、蜂窝织炎和与 GT 使用相关的泄漏等并发症很常见。GT 相关并发症可导致计划外儿科手术门诊或急诊 (ER) 就诊,这可能会耗费家庭大量时间并增加整体医疗保健成本。我们旨在确定与 CHD 婴儿 GT 手术后 2 周内和 GT 放置后 1 年出院回家后相关的 GT 并发症的因素。
我们使用胸外科医生协会数据库和一家三级儿童医院的电子病历进行了回顾性队列研究。我们确定了 2013 年 9 月至 2018 年 8 月期间接受 CHD 手术和 GT 手术的 <1 岁婴儿。测量了人口统计学、术前喂养方案、合并症和 GT 相关利用情况。记录了 GT 手术后 2 周内的术后 GT 并发症(例如 GT 蜂窝织炎、泄漏、移位、阻塞和肉芽组织)以及出院后 1 年内计划外儿科手术门诊或 ER 就诊情况。进行了双变量比较和多变量逻辑回归以评估与 GT 并发症和计划外门诊或 ER 就诊相关的因素。Kaplan-Meier 失效曲线检查了 ER/诊所就诊的时间。
在 152 名接受 CHD 然后 GT 手术的婴儿中,66%(N=101)有术后 GT 并发症。总体而言,出院后发现了 83 次计划外门诊就诊,其中 37%(N=31)是由于对肉芽组织的担忧。在 137 次 ER 就诊中,48%(N=66)是由于 GT 意外移位。与 GT 手术后 2 周内出院回家的婴儿相比,在 GT 手术后住院≥2 周的婴儿并发症更多(40.6%对 15.7%,P=0.002)。在接受 CHD 手术前接受口服营养的婴儿(38.6%对 60%,P<0.001)或患有单心室缺陷的婴儿(19.8%对 37.3%,P=0.02)的 GT 并发症更少。在调整了心脏异常类型后,在接受 CHD 手术前接受口服营养的婴儿 GT 并发症的可能性降低(优势比 OR 0.46;95%置信区间 CI:0.23-0.93)。Kaplan-Meier 失效曲线表明,在出院后 6 个月内,该队列中有 50%的患者出现导致计划外 ER/诊所就诊的并发症。
需要进行外科 GT 的 CHD 婴儿经常计划外到 ER 或儿科手术门诊就诊。心脏手术前的口服喂养与 GT 并发症较少有关。延长住院时间与更多的 GT 并发症相关。优化门诊护理和 GT 维持方面的家庭教育可能会减少这一高风险、依赖设备的婴儿人群的计划外就诊。