LaVasseur Corinne, Neukam Suvi, Kartika Thomas, Samuelson Bannow Bethany, Shatzel Joseph, DeLoughery Thomas G
Department of Medicine Oregon Health and Sciences University Portland Oregon USA.
Division of Internal Medicine Oregon Health and Sciences University Portland Oregon USA.
Res Pract Thromb Haemost. 2022 Aug 23;6(6):e12763. doi: 10.1002/rth2.12763. eCollection 2022 Aug.
Venous thromboses are well-established complications of hormonal therapy. Thrombosis risk is seen with both hormonal contraceptive agents and with hormone replacement therapy for menopause and gender transition. Over the past several decades, large epidemiological studies have helped better define these risks.
To review and discuss the differences in thrombosis risk of the many of hormonal preparations available as well as their interaction with patient-specific factors.
We conducted a narrative review of the available literature regarding venous thrombosis and hormonal therapies including for contraception, menopausal symptoms, and gender transition.
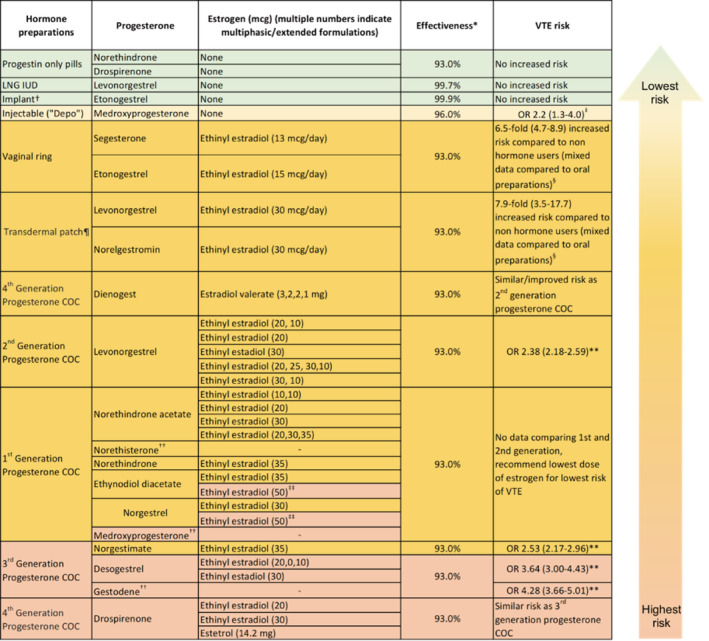
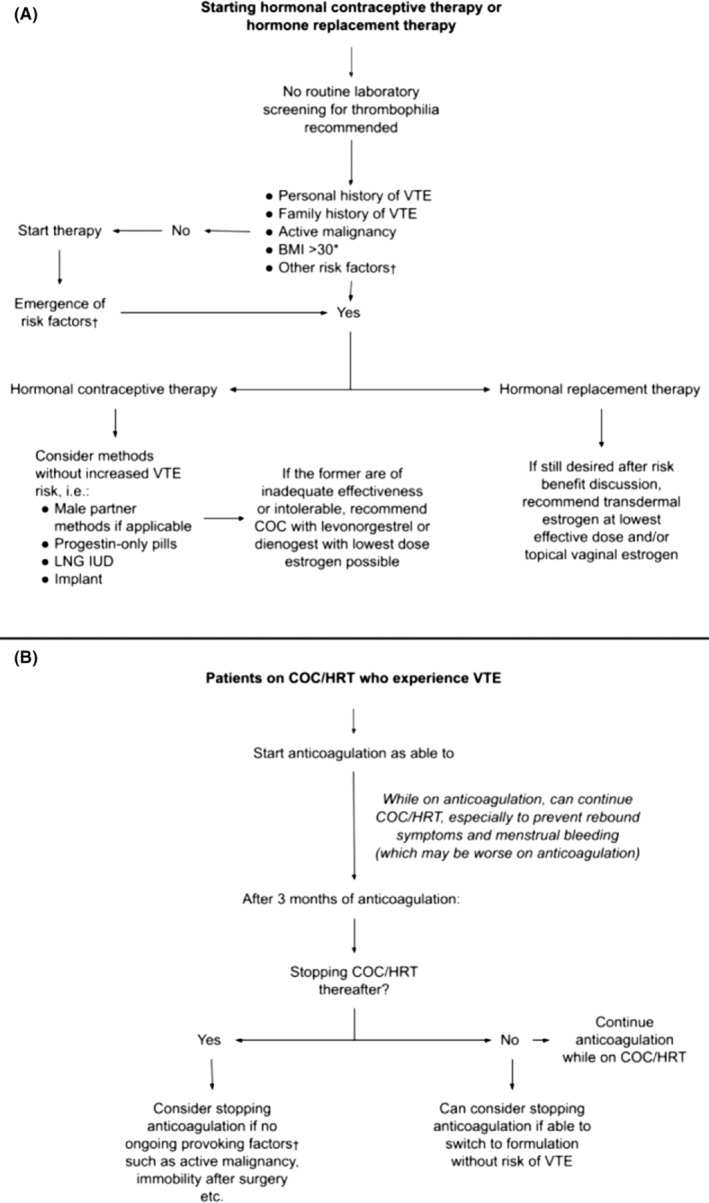
Thrombosis risk with estrogen-containing compounds increases with increasing systemic dose of estrogen. While progesterone-only-containing products are not associated with thrombosis, when paired with estrogen in combined oral contraceptives, the formulation of progesterone does impact the risk. These components, along with patient-specific factors, may influence the choice of hormonal preparation. For patients who develop thrombosis on hormonal treatment, anticoagulation is protective against future thrombosis. Duration of anticoagulation is dependent on ongoing and future hormone therapy choice. Finally, the optimal management of hormone therapy for individuals diagnosed with prothrombotic illnesses such as COVID-19 remains unclear.
When contemplating hormonal contraception or hormone replacement therapy, clinicians must consider a variety of factors including hormone type, dose, route, personal and family history of thrombosis, and other prothrombotic risk factors to make informed, personalized decisions regarding the risk of venous thrombosis.
静脉血栓形成是激素治疗公认的并发症。激素避孕药以及用于更年期和性别转换的激素替代疗法均存在血栓形成风险。在过去几十年中,大型流行病学研究有助于更好地界定这些风险。
回顾并讨论多种可用激素制剂的血栓形成风险差异及其与患者个体因素的相互作用。
我们对有关静脉血栓形成和激素疗法(包括用于避孕、更年期症状和性别转换的疗法)的现有文献进行了叙述性综述。
含雌激素化合物的血栓形成风险随雌激素全身剂量的增加而增加。仅含孕激素的产品与血栓形成无关,但在复方口服避孕药中与雌激素合用时,孕激素的配方确实会影响风险。这些因素以及患者个体因素可能会影响激素制剂的选择。对于在激素治疗期间发生血栓形成的患者,抗凝治疗可预防未来血栓形成。抗凝持续时间取决于正在进行的和未来的激素治疗选择。最后,对于被诊断患有血栓前疾病(如COVID-19)的个体,激素治疗的最佳管理仍不明确。
在考虑激素避孕或激素替代疗法时,临床医生必须考虑多种因素,包括激素类型、剂量、给药途径、个人和家族血栓形成史以及其他血栓前危险因素,以便就静脉血栓形成风险做出明智的个性化决策。