Zhao HanZheng, Chen Xingyu, Zhang WenHui, Cheng Die, Lu Yanjie, Wang Cheng, Li JunHu, You LiuPing, Yu JiaYong, Guo WenLong, Li YuHong, Huang YueNan
Department of General Surgery, The Second Affiliated Hospital of Harbin Medical University, Harbin, China.
College of Bioinformatics Science and Technology, Harbin Medical University, Harbin, China.
Front Surg. 2022 Aug 12;9:996844. doi: 10.3389/fsurg.2022.996844. eCollection 2022.
We investigated the clinical significance of preoperative pan-immune-inflammation value (PIV) in patients with colorectal cancer (CRC).
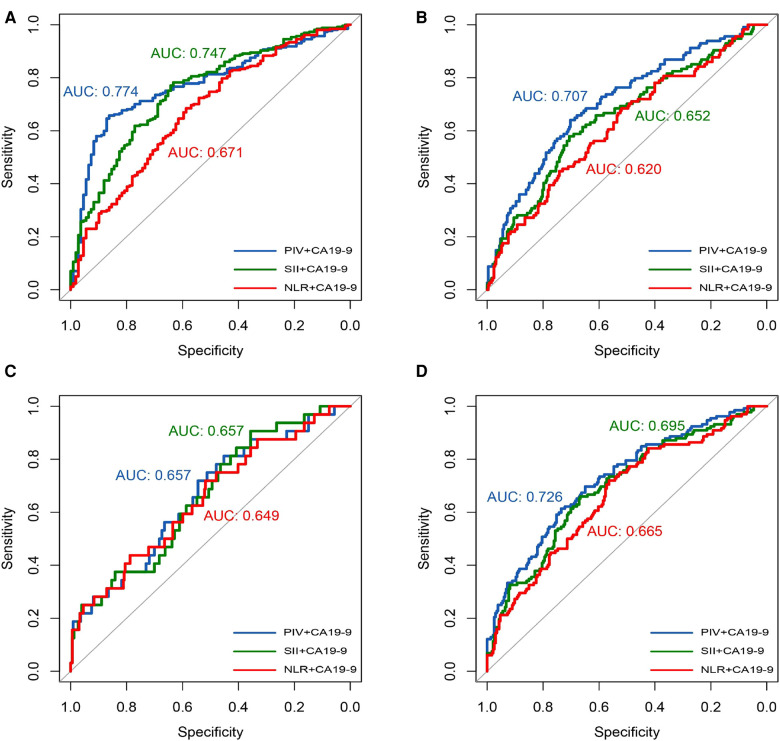
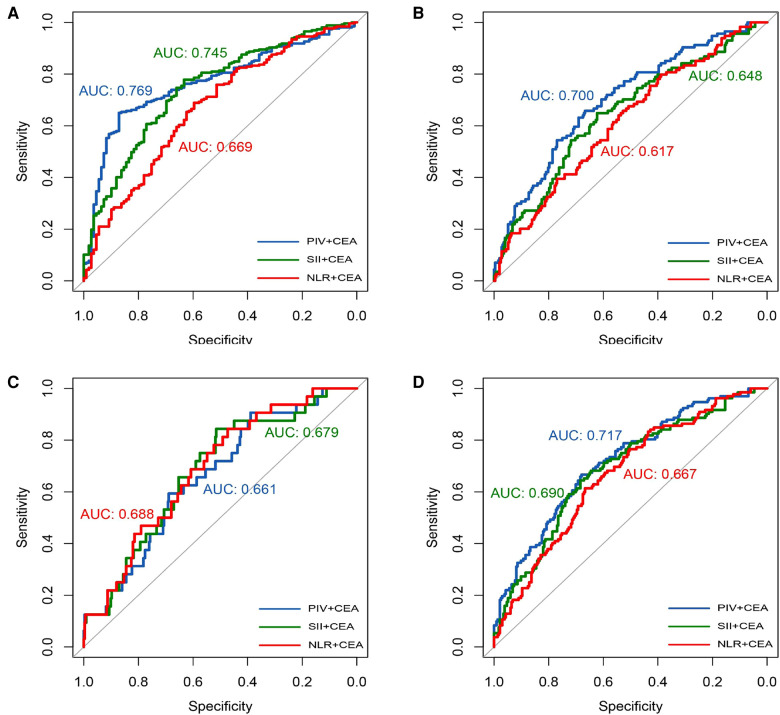
In this retrospective study, 366 cases who underwent surgery for CRC were enrolled. Their clinical data were collected. PIV was calculated with the formula PIV = [neutrophil count (10/L)× platelet count (10/L) × monocyte count (10/L) /lymphocyte count (10/L). Patients were divided into high PIV (> median PIV) and low PIV (< median PIV) groups. The relationship between PIV and clinicopathological features of CRC was investigated. Receiver operating characteristic (ROC) curve was plotted to indicate the value of immune-inflammatory biomarkers (IIBs) in predicting the TNM stage of CRC, and the area under the curve (AUC) was calculated to evaluate the actual clinical value of IIBs. AUC > 0.5 and closer to 1 indicated the better predictive efficacy. The influencing factors of PIV in CRC were analyzed.
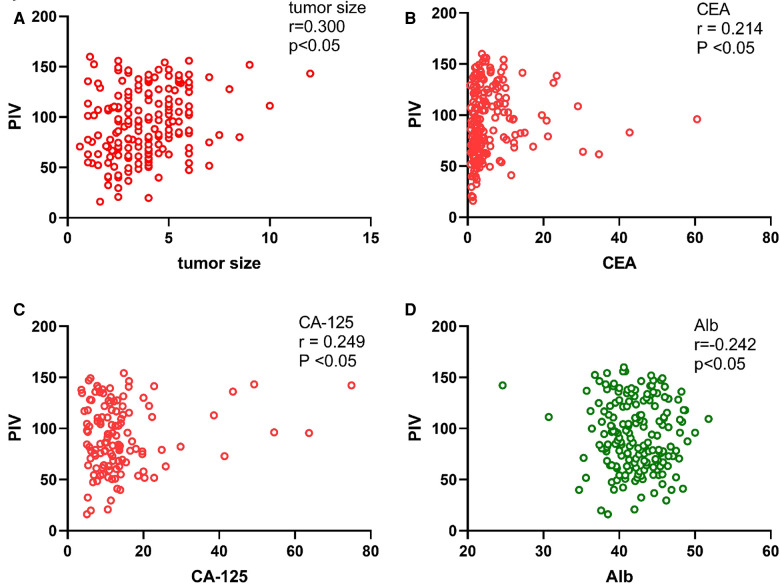
We found that PIV was positively correlated with tumor size ( = 0.300, < 0.05), carcinoembryonic antigen (CEA) ( = 0.214, < 0.05) and carbohydrate antigen 125 (CA-125) ( = 0.249, < 0.05), but negatively correlated with albumin (Alb) ( = -0.242, < 0.05). PIV was significantly different in patients with different tumor locations (left or right), surgical methods (laparotomy versus laparoscopic surgery) ( < 0.05), and patients with different pathological T stages, N-stage and TNM stages ( < 0.05). ROC curve analysis of IIBs showed the AUC of PIV was greater than other markers when combined with CEA or carbohydrate antigen 19-9 (CA19-9). Multivariate regression analysis identified T stage, CEA, Alb, and tumor size as the independent influential factors of PIV in CRC.
PIV is associated with the tumor stage in patients with CRC, which may be useful in preoperative assessment of CRC.
我们研究了术前全免疫炎症值(PIV)在结直肠癌(CRC)患者中的临床意义。
在这项回顾性研究中,纳入了366例行CRC手术的病例。收集他们的临床资料。PIV采用公式PIV = [中性粒细胞计数(10⁹/L)×血小板计数(10⁹/L)×单核细胞计数(10⁹/L)/淋巴细胞计数(10⁹/L)]计算。患者被分为高PIV(>中位数PIV)组和低PIV(<中位数PIV)组。研究PIV与CRC临床病理特征之间的关系。绘制受试者工作特征(ROC)曲线以表明免疫炎症生物标志物(IIBs)在预测CRC的TNM分期中的价值,并计算曲线下面积(AUC)以评估IIBs的实际临床价值。AUC > 0.5且越接近1表明预测效能越好。分析CRC中PIV的影响因素。
我们发现PIV与肿瘤大小(r = 0.300,P < 0.05)、癌胚抗原(CEA)(r = 0.214,P < 0.05)和糖类抗原125(CA - 125)(r = 0.249,P < 0.05)呈正相关,但与白蛋白(Alb)(r = -0.242,P < 0.05)呈负相关。不同肿瘤部位(左或右)、手术方式(开腹手术与腹腔镜手术)(P < 0.05)以及不同病理T分期, N分期和TNM分期的患者中PIV存在显著差异(P < 0.05)。IIBs的ROC曲线分析表明,当与CEA或糖类抗原19 - 9(CA19 - 9)联合使用时,PIV的AUC大于其他标志物。多因素回归分析确定T分期、CEA、Alb和肿瘤大小为CRC中PIV的独立影响因素。
PIV与CRC患者的肿瘤分期相关,这可能有助于CRC的术前评估。