Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, GA 30322.
Division of Infectious Diseases & International Health, University of Virginia, Charlottesville, VA 22908.
Proc Natl Acad Sci U S A. 2022 Sep 6;119(36):e2208972119. doi: 10.1073/pnas.2208972119. Epub 2022 Aug 29.
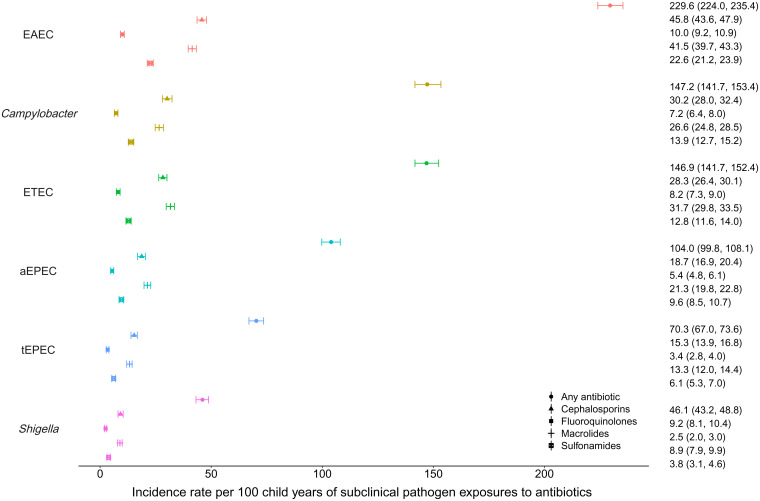
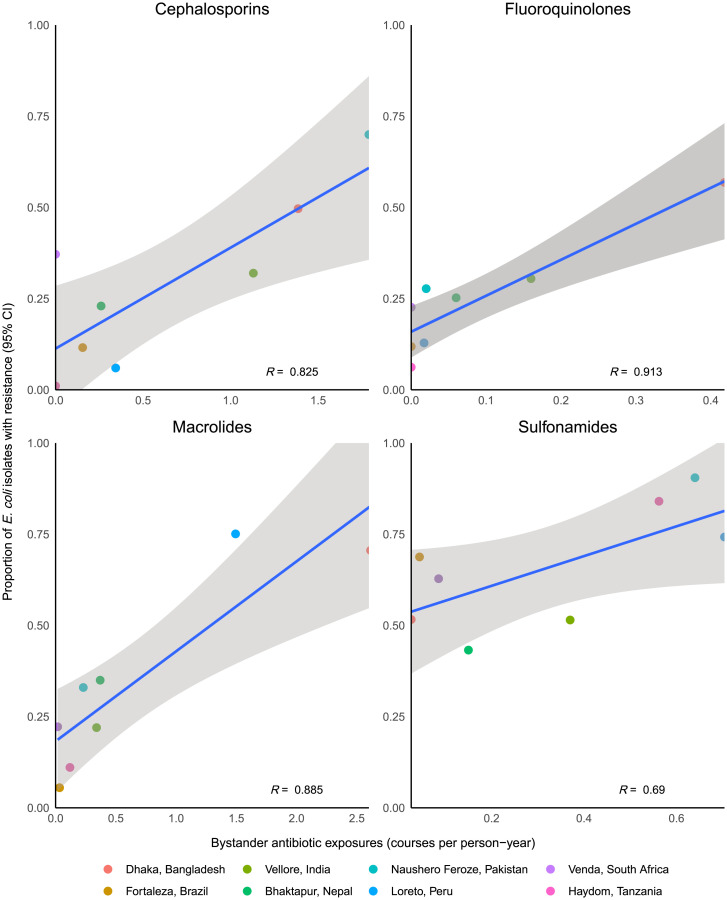
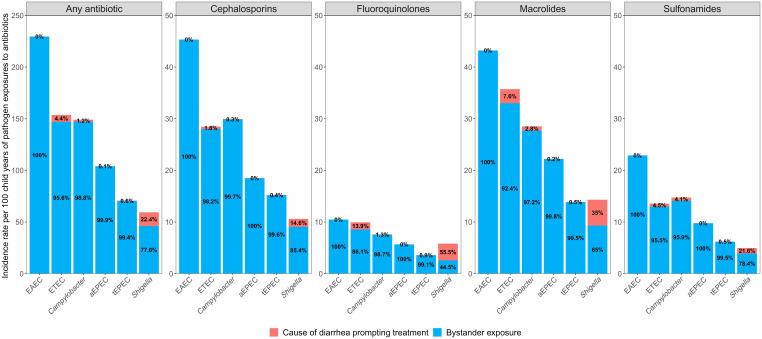
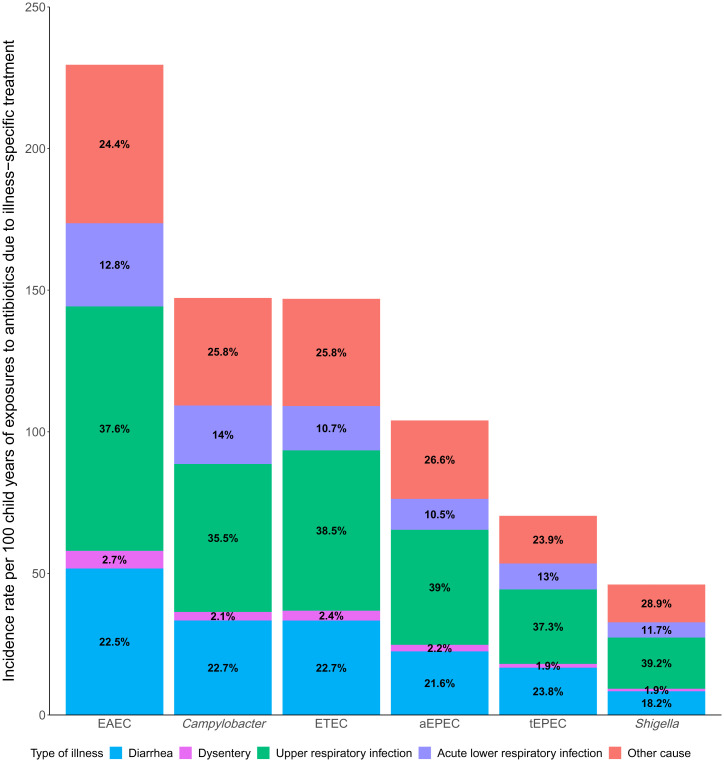
Children in low-resource settings carry enteric pathogens asymptomatically and are frequently treated with antibiotics, resulting in opportunities for pathogens to be exposed to antibiotics when not the target of treatment (i.e., bystander exposure). We quantified the frequency of bystander antibiotic exposures for enteric pathogens and estimated associations with resistance among children in eight low-resource settings. We analyzed 15,697 antibiotic courses from 1,715 children aged 0 to 2 y from the MAL-ED birth cohort. We calculated the incidence of bystander exposures and attributed exposures to respiratory and diarrheal illnesses. We associated bystander exposure with phenotypic susceptibility of E. coli isolates in the 30 d following exposure and at the level of the study site. There were 744.1 subclinical pathogen exposures to antibiotics per 100 child-years. Enteroaggregative was the most frequently exposed pathogen, with 229.6 exposures per 100 child-years. Almost all antibiotic exposures for (98.8%), enterotoxigenic (95.6%), and typical enteropathogenic (99.4%), and the majority for (77.6%), occurred when the pathogens were not the target of treatment. Respiratory infections accounted for half (49.9%) and diarrheal illnesses accounted for one-fourth (24.6%) of subclinical enteric bacteria exposures to antibiotics. Bystander exposure of to class-specific antibiotics was associated with the prevalence of phenotypic resistance at the community level. Antimicrobial stewardship and illness-prevention interventions among children in low-resource settings would have a large ancillary benefit of reducing bystander selection that may contribute to antimicrobial resistance.
在资源匮乏的环境中,儿童携带肠道病原体但无症状,并且经常接受抗生素治疗,导致病原体在未被治疗的情况下(即旁观者暴露)接触抗生素的机会增加。我们量化了肠道病原体旁观者抗生素暴露的频率,并估计了在八个资源匮乏的环境中儿童的抗生素耐药性的关联。我们分析了来自 MAL-ED 出生队列的 15697 个抗生素疗程,涉及 1715 名 0 至 2 岁的儿童。我们计算了旁观者暴露的发生率,并将暴露归因于呼吸道和腹泻疾病。我们将旁观者暴露与暴露后 30 天内大肠杆菌分离株的表型易感性以及研究地点的水平联系起来。每 100 名儿童年有 744.1 次亚临床病原体暴露于抗生素。肠聚集性是最常暴露的病原体,每 100 名儿童年有 229.6 次暴露。几乎所有针对 (98.8%)、肠毒性 (95.6%)和典型肠致病性 (99.4%)的抗生素暴露,以及针对 的大多数抗生素暴露 (77.6%),都发生在这些病原体不是治疗目标时。呼吸道感染占亚临床肠道细菌暴露于抗生素的一半(49.9%),腹泻病占四分之一(24.6%)。针对特定类别的抗生素的旁观者暴露与社区水平的表型耐药率有关。在资源匮乏的环境中,对儿童进行抗菌药物管理和疾病预防干预将具有很大的辅助益处,可以减少旁观者选择,这可能有助于抗菌药物耐药性的产生。