Division of Infectious Diseases & International Health, University of Virginia, Charlottesville, Virginia, United States of America.
Division of Epidemiology, School of Public Health, University of California, Berkeley, California, United States of America.
PLoS Med. 2023 Nov 22;20(11):e1004271. doi: 10.1371/journal.pmed.1004271. eCollection 2023 Nov.
Shigella is a leading cause of diarrhea and dysentery in children in low-resource settings, which is frequently treated with antibiotics. The primary goal of a Shigella vaccine would be to reduce mortality and morbidity associated with Shigella diarrhea. However, ancillary benefits could include reducing antibiotic use and antibiotic exposures for bystander pathogens carried at the time of treatment, specifically for fluoroquinolones and macrolides (F/M), which are the recommended drug classes to treat dysentery. The aim of the study was to quantify the reduction in Shigella attributable diarrhea, all diarrhea, and antibiotic use in the first 2 years of life that could be prevented by a Shigella vaccine.
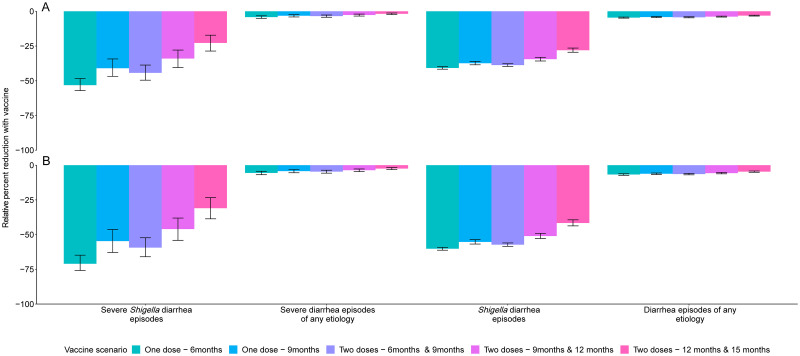
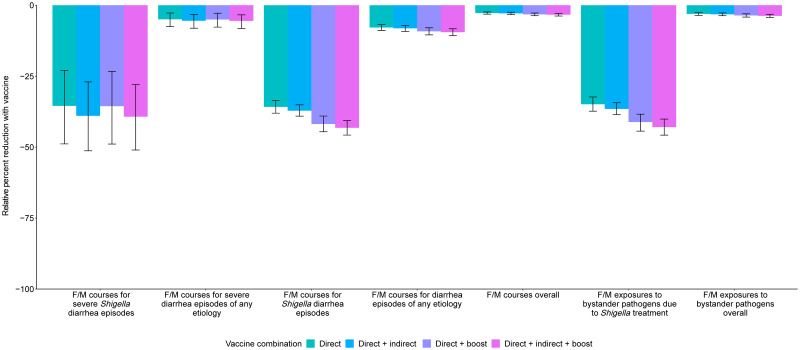
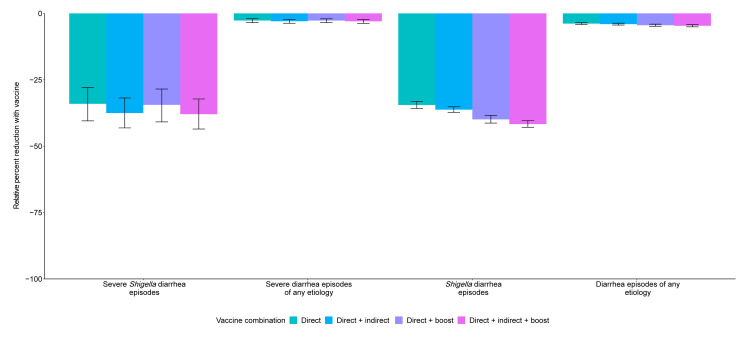
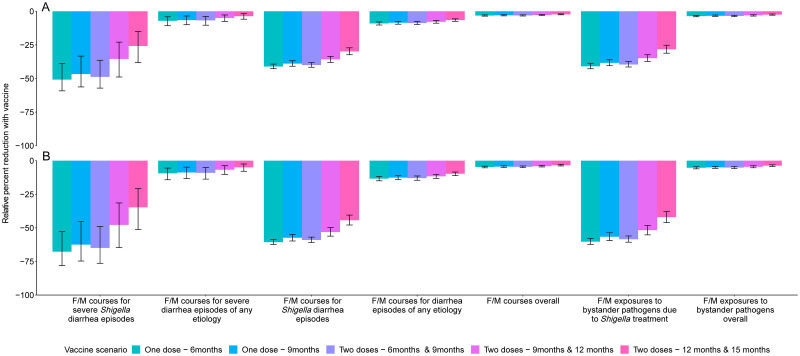
We used data from the Etiology, Risk Factors, and Interactions of Enteric Infections and Malnutrition and the Consequences for Child Health and Development (MAL-ED) study, a birth cohort study that followed 1,715 children with twice weekly surveillance for enteric infections, illnesses, and antibiotic use for the first 2 years of life from November 2009 to February 2014 at 8 sites. We estimated the impact of 2 one-dose (6 or 9 months) and 3 two-dose (6 and 9 months, 9 and 12 months, and 12 and 15 months) Shigella vaccines on diarrheal episodes, overall antibiotic use, and F/M use. Further, we considered additional protection through indirect and boosting effects. We used Monte Carlo simulations to estimate the absolute and relative reductions in the incidence of diarrhea and antibiotic use comparing each vaccination scenario to no vaccination. We analyzed 9,392 diarrhea episodes and 15,697 antibiotic courses among 1,715 children in the MAL-ED birth cohort study. There were 273.8 diarrhea episodes, 30.6 shigellosis episodes, and 457.6 antibiotic courses per 100 child-years. A Shigella vaccine with a mean vaccine efficacy of 60% against severe disease given at 9 and 12 months prevented 10.6 (95% CI [9.5, 11.5]) Shigella diarrhea episodes of any severity per 100 child-years (relative 34.5% reduction), 3.0 (95% CI [2.5, 3.5]) F/M courses for Shigella treatment per 100 child-years (relative 35.8% reduction), and 5.6 (95% CI [5.0, 6.3]) antibiotic courses of any drug class for Shigella treatment per 100 child-years (relative 34.5% reduction). This translated to a relative 3.8% reduction in all diarrhea, a relative 2.8% reduction in all F/M courses, a relative 3.1% reduction in F/M exposures to bystander pathogens, and a relative 0.9% reduction in all antibiotic courses. These results reflect Shigella incidence and antibiotic use patterns at the 8 MAL-ED sites and may not be generalizable to all low-resource settings.
Our simulation results suggest that a Shigella vaccine meeting WHO targets for efficacy could prevent about a third of Shigella diarrhea episodes, antibiotic use to treat shigellosis, and bystander exposures due to shigellosis treatment. However, the reductions in overall diarrhea episodes and antibiotic use are expected to be modest (<5%).
志贺氏菌是资源匮乏环境中儿童腹泻和痢疾的主要原因,常采用抗生素治疗。志贺氏菌疫苗的主要目标是降低与志贺氏菌腹泻相关的死亡率和发病率。然而,附带的益处可能包括减少抗生素的使用和治疗时同时携带的旁观者病原体(如氟喹诺酮类和大环内酯类)的抗生素暴露,氟喹诺酮类和大环内酯类是治疗痢疾的推荐药物类别。本研究的目的是量化通过志贺氏菌疫苗可预防的 2 岁以下儿童归因于志贺氏菌的腹泻、所有腹泻和抗生素使用的减少。
我们使用了 Etiology, Risk Factors, and Interactions of Enteric Infections and Malnutrition and the Consequences for Child Health and Development (MAL-ED) 研究的数据,这是一项出生队列研究,从 2009 年 11 月至 2014 年 2 月,在 8 个地点对 1715 名儿童进行了为期 2 年的每周两次的肠道感染、疾病和抗生素使用监测。我们估计了 2 剂(6 个月或 9 个月)和 3 剂(6 个月和 9 个月、9 个月和 12 个月、12 个月和 15 个月)志贺氏菌疫苗对腹泻发作、整体抗生素使用和氟喹诺酮类/大环内酯类(F/M)使用的影响。此外,我们还考虑了通过间接和增强效应的额外保护。我们使用蒙特卡罗模拟来估计比较每种疫苗接种方案与不接种疫苗的情况下,腹泻和抗生素使用的绝对和相对减少。我们分析了 1715 名儿童在 MAL-ED 出生队列研究中的 9392 次腹泻发作和 15697 次抗生素疗程。每 100 名儿童年有 273.8 次腹泻发作、30.6 次志贺菌病发作和 457.6 次抗生素疗程。在 9 个月和 12 个月时接种平均效力为 60%的志贺氏菌疫苗可预防 106 次(95%CI[9.5,11.5])任何严重程度的志贺氏菌腹泻发作(相对减少 34.5%)、3.0 次(95%CI[2.5,3.5])用于治疗志贺氏菌的 F/M 疗程(相对减少 35.8%)和 5.6 次(95%CI[5.0,6.3])用于治疗志贺氏菌的任何药物类别的抗生素疗程(相对减少 34.5%)。这相当于所有腹泻减少 3.8%、所有 F/M 课程减少 2.8%、F/M 暴露于旁观者病原体减少 3.1%和所有抗生素课程减少 0.9%。这些结果反映了 8 个 MAL-ED 地点的志贺氏菌发病率和抗生素使用模式,可能不适用于所有资源匮乏的环境。
我们的模拟结果表明,符合世卫组织疗效目标的志贺氏菌疫苗可能预防约三分之一的志贺氏菌腹泻发作、治疗志贺氏菌病的抗生素使用以及治疗志贺氏菌病导致的旁观者病原体暴露。然而,整体腹泻发作和抗生素使用的减少预计是适度的(<5%)。