Department of Public Health Sciences, University of Virginia, Charlottesville, Virginia, United States of America.
Division of Infectious Diseases & International Health, University of Virginia, Charlottesville, Virginia, United States of America.
PLoS Negl Trop Dis. 2020 Aug 17;14(8):e0008536. doi: 10.1371/journal.pntd.0008536. eCollection 2020 Aug.
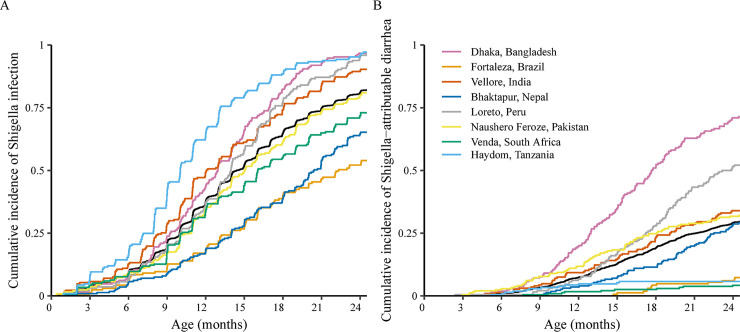
Culture-independent diagnostics have revealed a larger burden of Shigella among children in low-resource settings than previously recognized. We further characterized the epidemiology of Shigella in the first two years of life in a multisite birth cohort. We tested 41,405 diarrheal and monthly non-diarrheal stools from 1,715 children for Shigella by quantitative PCR. To assess risk factors, clinical factors related to age and culture positivity, and associations with inflammatory biomarkers, we used log-binomial regression with generalized estimating equations. The prevalence of Shigella varied from 4.9%-17.8% in non-diarrheal stools across sites, and the incidence of Shigella-attributable diarrhea was 31.8 cases (95% CI: 29.6, 34.2) per 100 child-years. The sensitivity of culture compared to qPCR was 6.6% and increased to 27.8% in Shigella-attributable dysentery. Shigella diarrhea episodes were more likely to be severe and less likely to be culture positive in younger children. Older age (RR: 1.75, 95% CI: 1.70, 1.81 per 6-month increase in age), unimproved sanitation (RR: 1.15, 95% CI: 1.03, 1.29), low maternal education (<10 years, RR: 1.14, 95% CI: 1.03, 1.26), initiating complementary foods before 3 months (RR: 1.10, 95% CI: 1.01, 1.20), and malnutrition (RR: 0.91, 95% CI: 0.88, 0.95 per unit increase in weight-for-age z-score) were risk factors for Shigella. There was a linear dose-response between Shigella quantity and myeloperoxidase concentrations. The burden of Shigella varied widely across sites, but uniformly increased through the second year of life and was associated with intestinal inflammation. Culture missed most clinically relevant cases of severe diarrhea and dysentery.
文化独立诊断方法揭示了资源匮乏环境中儿童的志贺菌负担比以前认识到的要大。我们进一步在多地点出生队列中描述了生命头两年志贺菌的流行病学。我们对 1715 名儿童的 41405 份腹泻和每月非腹泻粪便进行了定量 PCR 检测,以检测志贺菌。为了评估危险因素、与年龄和培养阳性相关的临床因素以及与炎症生物标志物的关联,我们使用了广义估计方程的对数二项式回归。各个地点非腹泻粪便中志贺菌的流行率从 4.9%到 17.8%不等,志贺菌引起的腹泻发病率为每 100 名儿童年 31.8 例(95%CI:29.6,34.2)。与 qPCR 相比,培养的敏感性为 6.6%,在志贺菌痢疾中增加到 27.8%。年龄较小的儿童发生志贺菌腹泻的可能性更大,更严重,培养阳性的可能性更小。年龄较大(RR:1.75,95%CI:1.70,1.81,每增加 6 个月年龄增加),卫生条件未改善(RR:1.15,95%CI:1.03,1.29),母亲受教育程度较低(<10 年,RR:1.14,95%CI:1.03,1.26),3 个月前开始添加补充食品(RR:1.10,95%CI:1.01,1.20)和营养不良(RR:0.91,95%CI:0.88,0.95,体重年龄 z 评分每增加一个单位)是志贺菌的危险因素。志贺菌数量与髓过氧化物酶浓度之间存在线性剂量反应关系。志贺菌的负担在各个地点差异很大,但在第二年呈递增趋势,并与肠道炎症有关。培养法错过了大多数具有临床意义的严重腹泻和痢疾病例。