Zhang Xu-Sheng, Ong Jason J, Macgregor Louis, Vilaplana Tatiana G, Heathcock Simone T, Mindlin Miranda, Weatherburn Peter, Hickson Ford, Edelstein Michael, Mandal Sema, Vickerman Peter
Statistics, Modelling and Economics, Data, Analytics & Surveillance, UK Health Security Agency, UK.
University of Bristol, Bristol, UK.
Lancet Reg Health Eur. 2022 Jun 17;19:100426. doi: 10.1016/j.lanepe.2022.100426. eCollection 2022 Aug.
Despite being vaccine-preventable, hepatitis A virus (HAV) outbreaks occur among men who have sex with men (MSM). We modelled the cost-effectiveness of vaccination strategies to prevent future outbreaks.
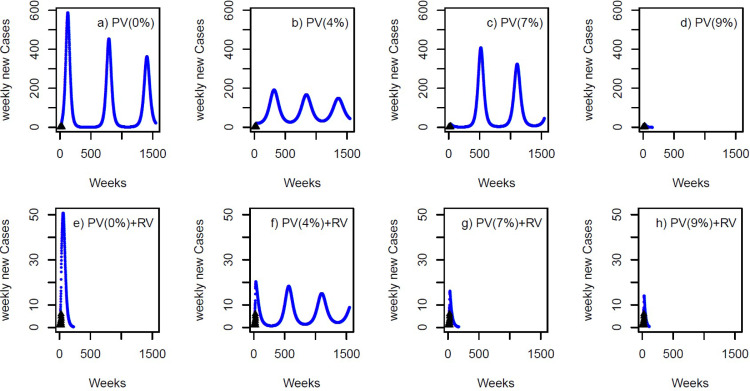
A HAV transmission model was calibrated to HAV outbreak data for MSM in England over 2016-2018, producing estimates for the basic reproduction number (R) and immunity levels (seroprevalence) post-outbreak. For a hypothetical outbreak in 2023 (same R and evolving immunity), the cost-effectiveness of pre-emptive (vaccination between outbreaks among MSM attending sexual health services (SHS)) and reactive (vaccination during outbreak among MSM attending SHS and primary care) vaccination strategies were modelled. Effectiveness in quality-adjusted life-years (QALYs) and costs were estimated (2017 UK pounds) from a societal perspective (10-year time horizon; 3% discount rate). The incremental cost-effectiveness ratio (ICER) was estimated.
R for the 2016-2018 outbreak was 3·19 (95% credibility interval (95%CrI) 2·87-3·46); seroprevalence among MSM increased to 70·4% (95%CrI 67·3-72·8%) post-outbreak. For our hypothetical HAV outbreak in 2023, pre-emptively vaccinating MSM over the preceding five-years was cost-saving (compared to no vaccination) if the yearly vaccine coverage rate among MSM attending SHS was <9·1%. Reactive vaccination was also cost-saving compared to no vaccination, but was dominated by pre-emptive vaccination if the yearly vaccination rate was >8%. If the pre-emptive yearly vaccination rate fell below this threshold, it became cost-saving to add reactive vaccination to pre-emptive vaccination.
Although highly transmissible, existing immunity limited the recent HAV outbreak among MSM in England. Pre-emptive vaccination between outbreaks, with reactive vaccination if indicated, is the best strategy for limiting future HAV outbreaks.
NIHR.
尽管甲型肝炎病毒(HAV)感染可通过疫苗预防,但男男性行为者(MSM)中仍会发生HAV疫情。我们对预防未来疫情的疫苗接种策略的成本效益进行了建模。
根据2016 - 2018年英格兰MSM的HAV疫情数据校准了HAV传播模型,得出疫情后基本再生数(R)和免疫水平(血清阳性率)的估计值。对于2023年的假设疫情(相同的R和不断变化的免疫力),对先发制人(在性健康服务机构(SHS)就诊的MSM在疫情间隔期进行疫苗接种)和反应性(在SHS和初级保健机构就诊的MSM在疫情期间进行疫苗接种)疫苗接种策略的成本效益进行了建模。从社会角度(10年时间范围;3%贴现率)估计了质量调整生命年(QALYs)的有效性和成本(2017年英镑)。估计了增量成本效益比(ICER)。
2016 - 2018年疫情的R为3.19(95%可信区间(95%CrI)2.87 - 3.46);疫情后MSM中的血清阳性率升至70.4%(95%CrI 67.3 - 72.8%)。对于我们假设的2023年HAV疫情,如果在性健康服务机构就诊的MSM的年度疫苗接种覆盖率<9.1%,在过去五年中对MSM进行先发制人疫苗接种是节省成本的(与不接种疫苗相比)。与不接种疫苗相比,反应性疫苗接种也节省成本,但如果年度疫苗接种率>8%,则被先发制人疫苗接种所主导。如果先发制人年度疫苗接种率低于此阈值,在先发制人疫苗接种基础上增加反应性疫苗接种就会节省成本。
尽管HAV传播性很强,但现有的免疫力限制了近期英格兰MSM中的HAV疫情。在疫情间隔期进行先发制人疫苗接种,并在必要时进行反应性疫苗接种,是限制未来HAV疫情的最佳策略。
英国国家卫生研究院(NIHR)