Nuffield Department of Primary Care Health Sciences, Radcliffe Observatory Quarter, University of Oxford, Oxford, OX2 6GG, UK.
Liverpool Reviews & Implementation Group, Institute of Population Health, University of Liverpool, Liverpool, L69 3BX, UK.
BMC Med. 2022 Aug 31;20(1):297. doi: 10.1186/s12916-022-02475-1.
Tackling problematic polypharmacy requires tailoring the use of medicines to individual circumstances and may involve the process of deprescribing. Deprescribing can cause anxiety and concern for clinicians and patients. Tailoring medication decisions often entails beyond protocol decision-making, a complex process involving emotional and cognitive work for healthcare professionals and patients. We undertook realist review to highlight and understand the interactions between different factors involved in deprescribing and to develop a final programme theory that identifies and explains components of good practice that support a person-centred approach to deprescribing in older patients with multimorbidity and polypharmacy.
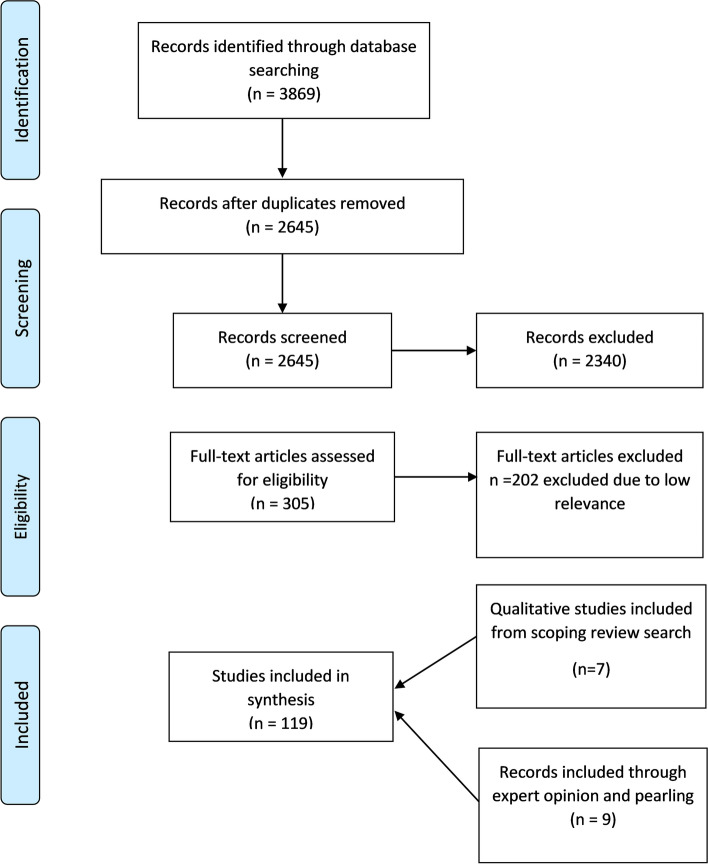
The realist approach involves identifying underlying causal mechanisms and exploring how, and under what conditions they work. We conducted a search of electronic databases which were supplemented by citation checking and consultation with stakeholders to identify other key documents. The review followed the key steps outlined by Pawson et al. and followed the RAMESES standards for realist syntheses.
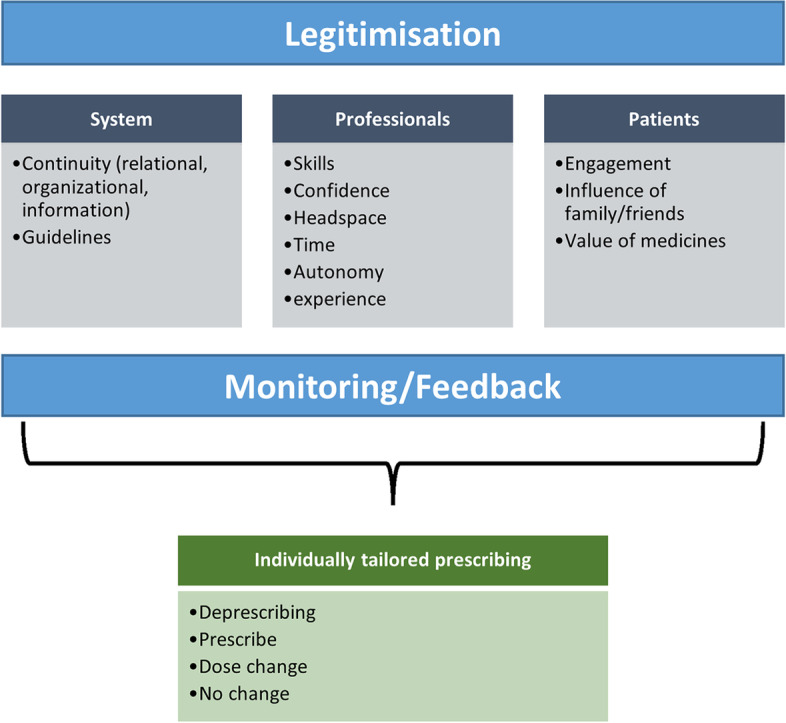
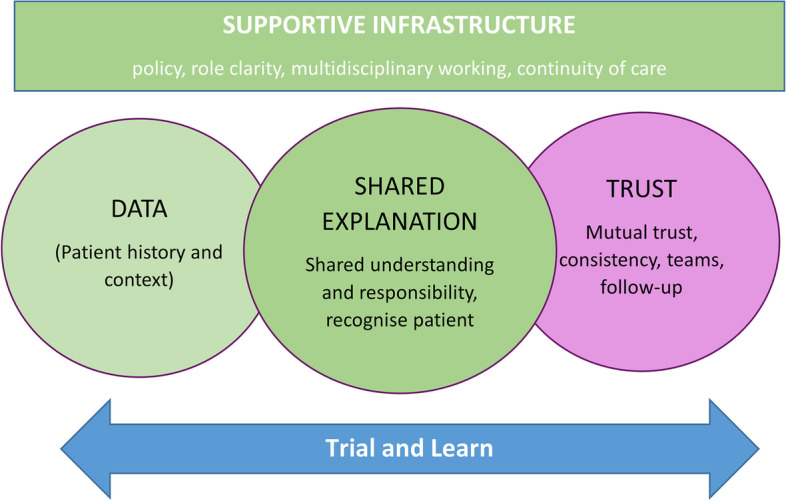
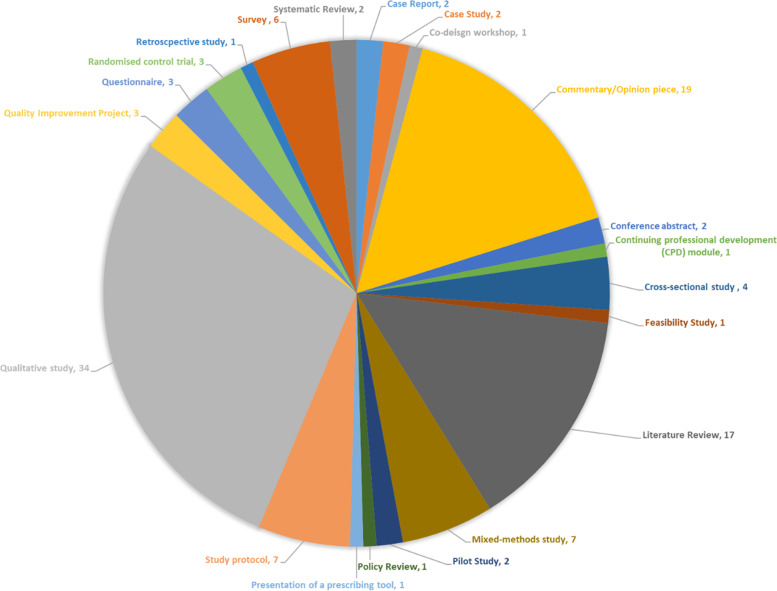
We included 119 included documents from which data were extracted to produce context-mechanism-outcome configurations (CMOCs) and a final programme theory. Our programme theory recognises that deprescribing is a complex intervention influenced by a multitude of factors. The components of our final programme theory include the following: a supportive infrastructure that provides clear guidance around professional responsibilities and that enables multidisciplinary working and continuity of care, consistent access to high-quality relevant patient contextual data, the need to support the creation of a shared explanation and understanding of the meaning and purpose of medicines and a trial and learn approach that provides space for monitoring and continuity. These components may support the development of trust which may be key to managing the uncertainty and in turn optimise outcomes. These components are summarised in the novel DExTruS framework.
Our findings recognise the complex interpretive practice and decision-making involved in medication management and identify key components needed to support best practice. Our findings have implications for how we design medication review consultations, professional training and for patient records/data management. Our review also highlights the role that trust plays both as a central element of tailored prescribing and a potential outcome of good practice in this area.
解决有问题的多种药物治疗需要根据个人情况调整药物的使用,可能涉及停药过程。停药可能会引起临床医生和患者的焦虑和担忧。调整药物决策通常需要超越方案决策,这是一个涉及医疗保健专业人员和患者情感和认知工作的复杂过程。我们进行了真实主义审查,以突出和理解与停药相关的不同因素之间的相互作用,并制定最终的计划理论,该理论确定并解释了支持以多药治疗和多病共存的老年患者为中心的停药方法的良好实践的组成部分。
真实主义方法涉及确定潜在的因果机制,并探索它们如何以及在何种条件下发挥作用。我们对电子数据库进行了搜索,并通过引用检查和与利益相关者的协商来补充其他关键文件。该审查遵循了 Pawson 等人概述的关键步骤,并遵循了真实主义综合的 RAMESES 标准。
我们纳入了 119 篇纳入文献,从中提取数据以生成背景-机制-结果配置(CMOC)和最终计划理论。我们的计划理论认识到,停药是一种受到多种因素影响的复杂干预措施。我们最终计划理论的组成部分包括以下内容:一个支持性的基础设施,提供有关专业责任的明确指导,使多学科合作和护理连续性成为可能,持续获得高质量的相关患者背景数据,支持创建对药物的意义和目的的共同解释和理解的需求,以及试验和学习方法,为监测和连续性提供空间。这些组成部分可能有助于建立信任,这可能是管理不确定性的关键,从而优化结果。这些组成部分在新颖的 DExTruS 框架中进行了总结。
我们的研究结果认识到药物管理中涉及的复杂解释实践和决策,并确定了支持最佳实践所需的关键组成部分。我们的研究结果对我们如何设计药物审查咨询、专业培训以及患者记录/数据管理具有影响。我们的审查还强调了信任在量身定制的处方中作为核心要素以及在该领域良好实践中的潜在结果所起的作用。