Seeley Elizabeth A, Zimmer Markie, Berghea Ramona
Internal Medicine, Beaumont Health, Royal Oak, USA.
Cureus. 2022 Jul 26;14(7):e27313. doi: 10.7759/cureus.27313. eCollection 2022 Jul.
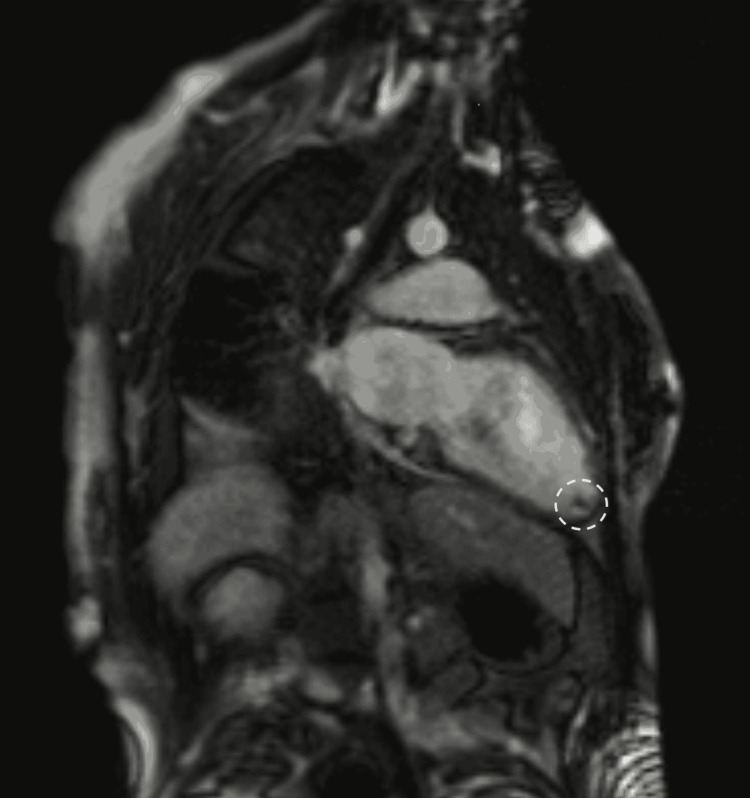
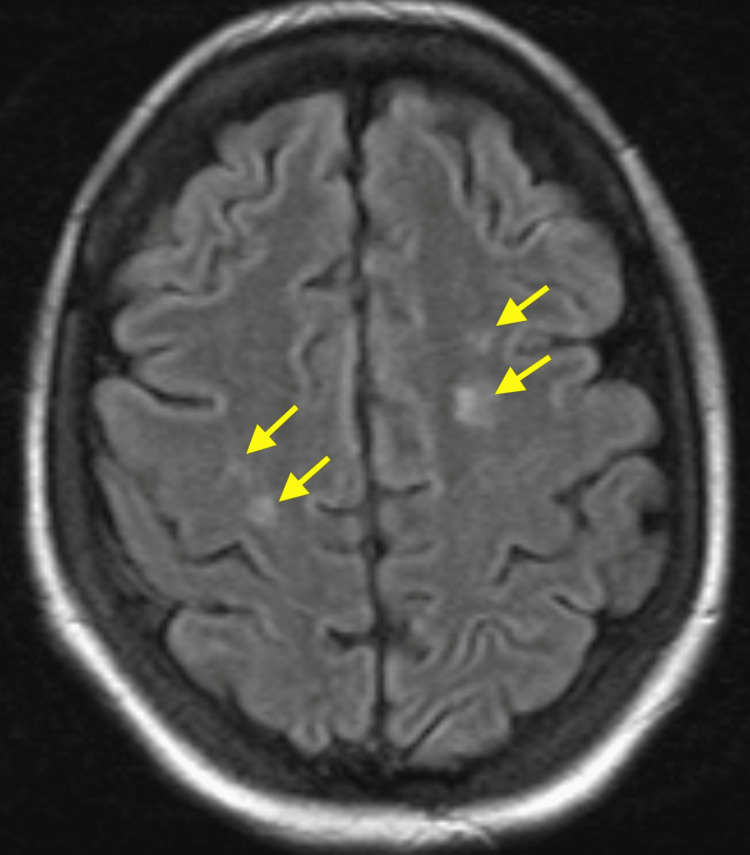
In this report, we describe the case of a woman with suspected COVID-19 immunization-induced probable catastrophic antiphospholipid syndrome. The patient is a 35-year-old female with a past medical history significant for antiphospholipid syndrome, not on anticoagulation, who presented with a 5-day history of abdominal pain and distention, nausea, vomiting, and shortness of breath. She had received her first dose of the Pfizer COVID-19 vaccine one day prior to the onset of symptoms. After extensive workup at an outside hospital, she was found to be in acute heart failure exacerbated by severe mitral and tricuspid regurgitation. She was transferred to our hospital for escalation of care. EKG showed evidence of prior inferior and septal myocardial infarction. Transesophageal echocardiogram (TEE) showed reduced ejection fraction, severe mitral and tricuspid regurgitation, and a left ventricular thrombus. Cardiac MRI showed subendocardial late gadolinium enhancement indicative of ischemia. However, CTA of the coronary vessels showed no signs of obstruction. Therefore, her acute heart failure was thought to be due to small vessel thrombosis secondary to antiphospholipid syndrome. During admission, she had several absence seizure-like episodes. CT head showed several hypodensities of the deep white matter and brain MRI demonstrated multiple hyperintense T2 FLAIR signal foci with restriction diffusion and enhancement involving the cerebral hemisphere, consistent with subacute strokes attributed to being secondary to antiphospholipid syndrome or embolic from the left ventricular thrombus. She was treated with heparin for suspected catastrophic antiphospholipid syndrome and high-dose corticosteroid therapy for concomitant Systemic Lupus Erythematosus (SLE). She was discharged in a stable condition.
在本报告中,我们描述了一例疑似因接种新冠病毒疫苗诱发可能的灾难性抗磷脂综合征的女性病例。患者为一名35岁女性,既往有抗磷脂综合征病史,未接受抗凝治疗,出现腹痛、腹胀、恶心、呕吐及呼吸急促5天。症状出现前一天,她接种了第一剂辉瑞新冠病毒疫苗。在外院进行全面检查后,发现她因严重二尖瓣和三尖瓣反流而加重了急性心力衰竭。她被转至我院接受进一步治疗。心电图显示有既往下壁和间隔心肌梗死的迹象。经食管超声心动图(TEE)显示射血分数降低、严重二尖瓣和三尖瓣反流以及左心室血栓。心脏磁共振成像显示心内膜下晚期钆增强,提示缺血。然而,冠状动脉CT血管造影未显示梗阻迹象。因此,她的急性心力衰竭被认为是抗磷脂综合征继发的小血管血栓形成所致。住院期间,她出现了几次类似失神发作的情况。头颅CT显示深部白质有几处低密度影,脑部磁共振成像显示多个T2液体衰减反转恢复序列高信号灶,伴有扩散受限和强化,累及大脑半球,符合抗磷脂综合征继发或左心室血栓栓塞所致的亚急性中风。她因疑似灾难性抗磷脂综合征接受肝素治疗,并因合并系统性红斑狼疮(SLE)接受大剂量皮质类固醇治疗。她出院时病情稳定。