Department of General Paediatrics, Erasmus MC-Sophia Children's Hospital, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Department of Paediatrics, Erasmus MC-Sophia Children's Hospital, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Pediatr Crit Care Med. 2022 Dec 1;23(12):e543-e554. doi: 10.1097/PCC.0000000000003056. Epub 2022 Aug 31.
We aimed to describe the variation of hemostasis proteins in children with bacterial infections due to different pathogens ( Neisseria meningitidis, Streptococcus pneumoniae, Staphylococcus aureus , and group A streptococcus [GAS]) and to study hemostasis proteins in relation to mortality.
Preplanned analysis in prospective cohort study.
Hospitals in five European countries (Austria, The Netherlands, Spain, Switzerland, and the United Kingdom).
Admitted children (2012-2016) with community-acquired infections due to meningococci ( n = 83), pneumococci ( n = 64), S. aureus (n = 50), and GAS ( n = 44) with available serum samples collected less than 48 hours after admission.
None.
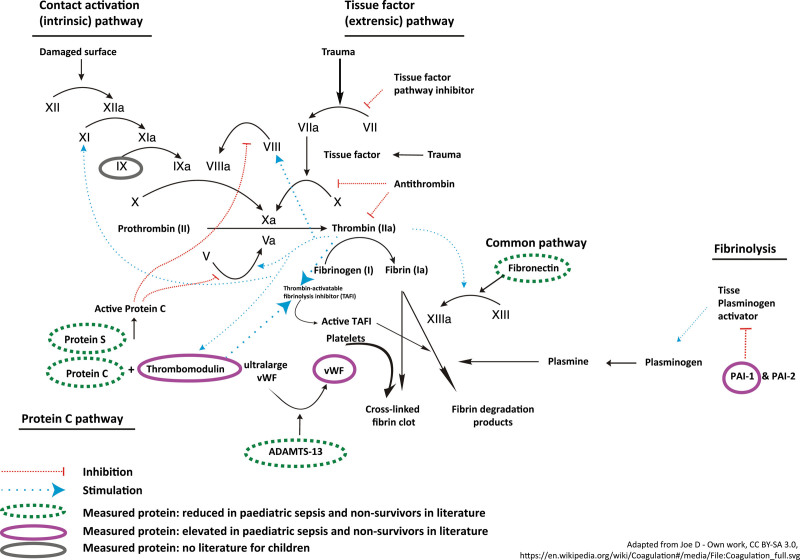
Fibronectin, plasminogen activator inhibitor type 1 (PAI-1), thrombomodulin, and a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS-13) were measured in serum in 2019-2020. Additionally, von Willebrand factor, protein C, protein S, and factor IX were measured in citrate plasma available from a subset of patients. Outcome measures included in-hospital mortality and disease severity (need for ventilation/inotropes, Pediatric Index of Mortality score).Of 241 children, 21 (8.7%) died and 177 (73.5%) were admitted to PICU. Mortality rate was similar for the pathogen groups. Levels of fibronectin and thrombomodulin differed for the different pathogens ( p < 0.05). Fibronectin levels were lower in GAS infections than in S. pneumoniae and S. aureus infections but did not differ from meningococcal infections. Thrombomodulin levels in meningococcal infections were higher than in S. aureus and pneumococcal infections. Overall, the area under the curve for mortality was 0.81 (95% CI, 0.70-0.92) for thrombomodulin and 0.78 (95% CI, 0.69-0.88) for ADAMTS-13. The association of each hemostasis protein did not vary across pathogens for any of the outcome measures.
Hemostatic disturbances in childhood bacterial infections are not limited to meningococcal sepsis but occur with a comparable severity across nonmeningococcal infections. High thrombomodulin and high ADAMTS-13 had good discriminative ability for mortality. Our results emphasize the importance of hemostatic disturbances in meningococcal and nonmeningococcal pediatric bacterial infections.
本研究旨在描述因不同病原体(脑膜炎奈瑟菌、肺炎链球菌、金黄色葡萄球菌和 A 组链球菌)引起的细菌性感染患儿的止血蛋白变化,并研究止血蛋白与死亡率的关系。
前瞻性队列研究的预分析。
欧洲五个国家(奥地利、荷兰、西班牙、瑞士和英国)的医院。
2012-2016 年间因脑膜炎球菌(n=83)、肺炎球菌(n=64)、金黄色葡萄球菌(n=50)和 A 组链球菌(n=44)感染而入院的社区获得性感染患儿,且入院后 48 小时内采集了血清样本。
无。
2019-2020 年,检测了血清中的纤维连接蛋白、纤溶酶原激活物抑制剂 1(PAI-1)、血栓调节蛋白和 a 型血小板反应蛋白 13(ADAMTS-13)。此外,还在部分患者的柠檬酸盐血浆中检测了血管性血友病因子、蛋白 C、蛋白 S 和因子 IX。观察指标包括院内死亡率和疾病严重程度(需要通气/正性肌力药、儿科死亡率评分)。241 例患儿中,21 例(8.7%)死亡,177 例(73.5%)入住 PICU。不同病原体组的死亡率相似。纤维连接蛋白和血栓调节蛋白水平因病原体不同而不同(p<0.05)。与肺炎链球菌和金黄色葡萄球菌感染相比,GAS 感染时纤维连接蛋白水平较低,但与脑膜炎奈瑟菌感染无差异。脑膜炎奈瑟菌感染时血栓调节蛋白水平高于金黄色葡萄球菌和肺炎链球菌感染。总体而言,血栓调节蛋白的死亡率曲线下面积为 0.81(95%CI,0.70-0.92),ADAMTS-13 为 0.78(95%CI,0.69-0.88)。对于任何观察指标,每种止血蛋白的相关性在不同病原体之间均无差异。
儿童细菌性感染中的止血紊乱不仅限于脑膜炎球菌性败血症,而且在非脑膜炎球菌感染中也具有相似的严重程度。高血栓调节蛋白和高 ADAMTS-13 对死亡率具有良好的鉴别能力。本研究结果强调了脑膜炎球菌和非脑膜炎球菌性儿童细菌性感染中止血紊乱的重要性。