Department of Sports Medicine, Norwegian School of Sport Sciences, PO Box 4014, Ullevål stadion, 0806, Oslo, Norway.
Department of Obstetrics and Gynaecology, Akershus University Hospital, Lørenskog, Norway.
Int Urogynecol J. 2022 Dec;33(12):3455-3464. doi: 10.1007/s00192-022-05334-y. Epub 2022 Sep 1.
To date there has been scant knowledge on the natural recovery of the pelvic floor muscles (PFMs) after childbirth. The aims of the present study were to investigate whether PFM variables at 6 and 12 months postpartum had returned to mid-pregnancy levels and assess risk factors for reduced recovery at 12 months postpartum.
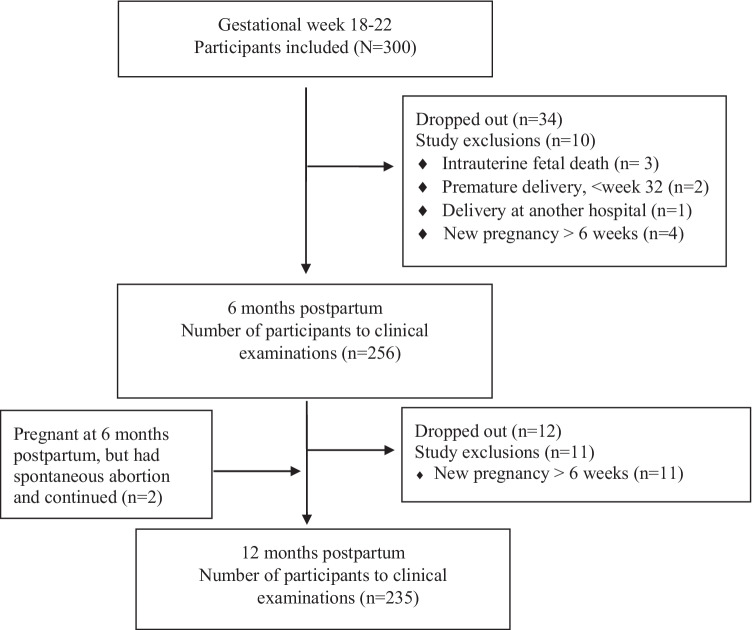
This was a prospective cohort study following 235 nulliparous pregnant women from mid-pregnancy to 12 months postpartum. Vaginal resting pressure (VRP), PFM strength and endurance were assessed by manometry at 22 weeks, 6 and 12 months postpartum. Multiple linear regression was used to address factors influencing PFM variables beyond birth mode.
Cesarean section was protective for change in PFM variables. From mid-pregnancy to 12 months postpartum there was a 20% reduction in VRP (p<0.001) and a 7.5 % reduction in PFM strength (p=0.007), and an increase of 9% in PFM endurance (p=0.002) in the normal vaginal birth. The instrumental vaginal group had a decline in VRP of 21% (p<0.001) and PFM strength of 15% (p=0.011), but no significant change in PFM endurance. Higher BMI at 12 months postpartum, longer second stage of labor, and major tears of the levator ani muscle had a negative influence on the PFM recovery beyond delivery mode.
At 12 months postpartum following vaginal delivery, the PFMs are not fully recovered compared with mid-pregnancy values. More follow-up physical therapy may be warranted in the postpartum period, especially for women with complicated vaginal births and higher BMI.
迄今为止,关于产后盆底肌(PFMs)自然恢复的知识还很少。本研究旨在探讨产后 6 个月和 12 个月时 PFM 变量是否已恢复至妊娠中期水平,并评估产后 12 个月时恢复情况不佳的危险因素。
这是一项前瞻性队列研究,共纳入 235 名初产妇,从妊娠中期至产后 12 个月进行随访。在 22 周、产后 6 个月和 12 个月时通过压力测定法评估阴道静息压(VRP)、PFM 力量和耐力。采用多元线性回归分析探讨影响 PFM 变量的因素。
剖宫产对 PFM 变量的变化具有保护作用。从中孕期到产后 12 个月,VRP 降低了 20%(p<0.001),PFM 力量降低了 7.5%(p=0.007),PFM 耐力增加了 9%(p=0.002)。在正常阴道分娩组中,VRP 下降了 21%(p<0.001),PFM 力量下降了 15%(p=0.011),但 PFM 耐力无显著变化。产后 12 个月时 BMI 较高、第二产程较长以及肛提肌撕裂较大,除分娩方式外,对 PFM 恢复也有负面影响。
产后 12 个月时,与妊娠中期相比,阴道分娩后 PFMs 并未完全恢复。尤其是对于分娩复杂的女性和 BMI 较高的女性,产后可能需要更多的物理治疗。