Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, CDC.
MMWR Surveill Summ. 2022 Sep 2;71(8):1-35. doi: 10.15585/mmwr.ss7108a1.
PROBLEM/CONDITION: Malaria in humans is caused by intraerythrocytic protozoa of the genus Plasmodium. These parasites are transmitted by the bite of an infective female Anopheles species mosquito. Most malaria infections in the United States and its territories occur among persons who have traveled to regions with ongoing malaria transmission. However, among persons who have not traveled out of the country, malaria is occasionally acquired through exposure to infected blood or tissues, congenital transmission, nosocomial exposure, or local mosquitoborne transmission. Malaria surveillance in the United States and its territories provides information on its occurrence (e.g., temporal, geographic, and demographic), guides prevention and treatment recommendations for travelers and patients, and facilitates rapid transmission control measures if locally acquired cases are identified.
This report summarizes confirmed malaria cases in persons with onset of illness in 2018 and trends in previous years.
Malaria cases diagnosed by blood smear microscopy, polymerase chain reaction, or rapid diagnostic tests are reported to local and state health departments through electronic laboratory reports or by health care providers or laboratory staff members directly reporting to CDC or health departments. Case investigations are conducted by local and state health departments, and reports are transmitted to CDC through the National Malaria Surveillance System (NMSS), the National Notifiable Diseases Surveillance System (NNDSS), or direct CDC clinical consultations. CDC reference laboratories provide diagnostic assistance and conduct antimalarial drug resistance marker testing on blood specimens submitted by health care providers or local or state health departments. This report summarizes data from the integration of all cases from NMSS and NNDSS, CDC clinical consultations, and CDC reference laboratory reports.
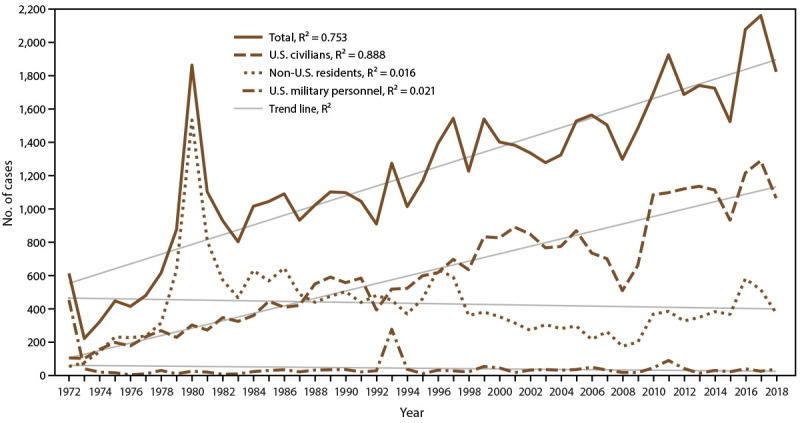
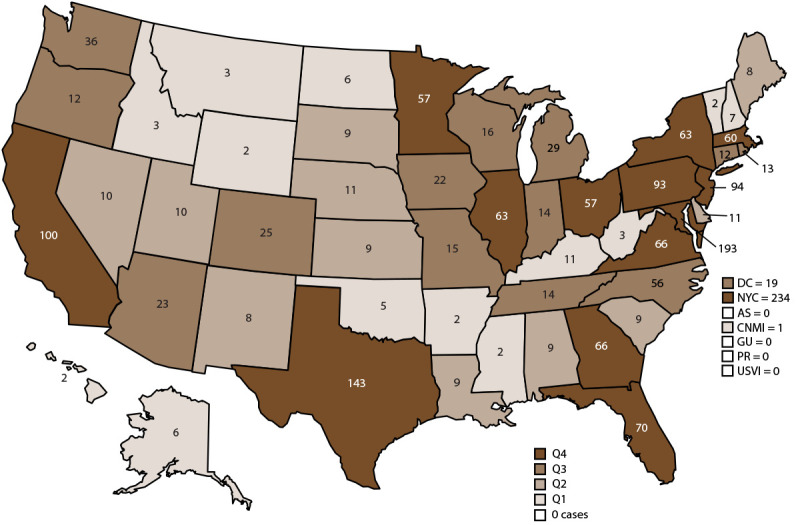
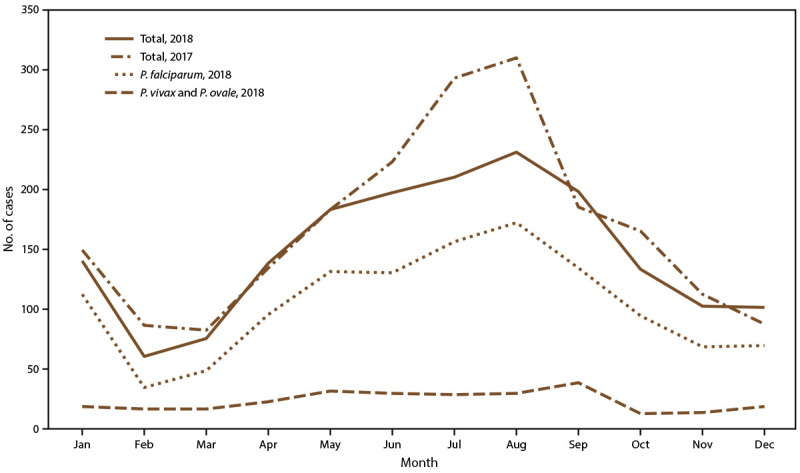
CDC received reports of 1,823 confirmed malaria cases with onset of symptoms in 2018, including one cryptic case and one case acquired through a bone marrow transplant. The number of cases reported in 2018 is 15.6% fewer than in 2017. The number of cases diagnosed in the United States and its territories has been increasing since the mid-1970s; the number of cases reported in 2017 was the highest since 1972. Of the cases in 2018, a total of 1,519 (85.0%) were imported cases that originated from Africa; 1,061 (69.9%) of the cases from Africa were from West Africa, a similar proportion to what was observed in 2017. Among all cases, P. falciparum accounted for most infections (1,273 [69.8%]), followed by P. vivax (173 [9.5%]), P. ovale (95 [5.2%]), and P. malariae (48 [2.6%]). For the first time since 2008, an imported case of P. knowlesi was identified in the United States and its territories. Infections by two or more species accounted for 17 cases (<1.0%). The infecting species was not reported or was undetermined in 216 cases (11.9%). Most patients (92.6%) had symptom onset <90 days after returning to the United States or its territories from a country with malaria transmission. Of the U.S. civilian patients who reported reason for travel, 77.0% were visiting friends and relatives. Chemoprophylaxis with antimalarial medications are recommended for U.S. residents to prevent malaria while traveling in countries where it is endemic. Fewer U.S. residents with imported malaria reported taking any malaria chemoprophylaxis in 2018 (24.5%) than in 2017 (28.4%), and adherence was poor among those who took chemoprophylaxis. Among the 864 U.S. residents with malaria for whom information on chemoprophylaxis use and travel region were known, 95.0% did not adhere to or did not take a CDC-recommended chemoprophylaxis regimen. Among 683 women with malaria, 19 reported being pregnant. Of these, 11 pregnant women were U.S. residents, and one of whom reported taking chemoprophylaxis to prevent malaria but her adherence to chemoprophylaxis was not reported. Thirty-eight (2.1%) malaria cases occurred among U.S. military personnel in 2018, more than in 2017 (26 [1.2%]). Among all reported malaria cases in 2018, a total of 251 (13.8%) were classified as severe malaria illness, and seven persons died from malaria. In 2018, CDC analyzed 106 P. falciparum-positive and four P. falciparum mixed species specimens for antimalarial resistance markers (although certain loci were untestable in some specimens); identification of genetic polymorphisms associated with resistance to pyrimethamine were found in 99 (98.0%), to sulfadoxine in 49 (49.6%), to chloroquine in 50 (45.5%), and to mefloquine in two (2.0%); no specimens tested contained a marker for atovaquone or artemisinin resistance.
The importation of malaria reflects the overall trends in global travel to and from areas where malaria is endemic, and 15.6% fewer cases were imported in 2018 compared with 2017. Of imported cases, 59.3% were among persons who had traveled from West Africa. Among U.S. civilians, visiting friends and relatives was the most common reason for travel (77.1%).
The best way for U.S. residents to prevent malaria is to take chemoprophylaxis medication before, during, and after travel to a country where malaria is endemic. Adherence to recommended malaria prevention strategies among U.S. travelers would reduce the number of imported cases. Reported reasons for nonadherence include prematurely stopping after leaving the area where malaria was endemic, forgetting to take the medication, and experiencing a side effect. Health care providers can make travelers aware of the risks posed by malaria and incorporate education to motivate them to be adherent to chemoprophylaxis. Malaria infections can be fatal if not diagnosed and treated promptly with antimalarial medications appropriate for the patient's age, pregnancy status, medical history, the likely country of malaria acquisition, and previous use of antimalarial chemoprophylaxis. Antimalarial use for chemoprophylaxis and treatment should be determined by the CDC guidelines, which are frequently updated. In April 2019, intravenous (IV) artesunate became the first-line medication for treatment of severe malaria in the United States and its territories. Artesunate was approved by the Food and Drug Administration (FDA) in 2020 and is commercially available (Artesunate for Injection) from major U.S. drug distributors (https://amivas.com). Stocking IV artesunate locally allows for immediate treatment of severe malaria once diagnosed and provides patients with the best chance of a complete recovery and no sequelae. With commercial IV artesunate now available, CDC will discontinue distribution of non-FDA-approved IV artesunate under an investigational new drug protocol on September 30, 2022. Detailed recommendations for preventing malaria are online at https://www.cdc.gov/malaria/travelers/drugs.html. Malaria diagnosis and treatment recommendations are also available online at https://www.cdc.gov/malaria/diagnosis_treatment. Health care providers who have sought urgent infectious disease consultation and require additional assistance on diagnosis and treatment of malaria can call the Malaria Hotline 9:00 a.m.-5:00 p.m. Eastern Time, Monday-Friday, at 770-488-7788 or 855-856-4713 or after hours for urgent inquiries at 770-488-7100. Persons submitting malaria case reports (care providers, laboratories, and state and local public health officials) should provide complete information because incomplete reporting compromises case investigations and public health efforts to prevent future infections and examine trends in malaria cases. Molecular surveillance of antimalarial drug resistance markers enables CDC to track, guide treatment, and manage drug resistance in malaria parasites both domestically and globally. A greater proportion of specimens from domestic malaria cases are needed to improve the completeness of antimalarial drug resistance analysis; therefore, CDC requests that blood specimens be submitted for any case of malaria diagnosed in the United States and its territories.
问题/状况:人类疟疾是由疟原虫属的红细胞内原生动物引起的。这些寄生虫通过感染性雌性按蚊物种的蚊子叮咬传播。美国及其领土上大多数疟疾病例发生在前往疟疾持续传播地区的人身上。然而,在没有出国旅行的人群中,疟疾偶尔会通过接触受感染的血液或组织、先天传播、院内暴露或当地蚊媒传播而获得。美国及其领土的疟疾监测提供了关于其发生情况的信息(例如,时间、地理和人口统计学),为旅行者和患者的预防和治疗建议提供指导,并在发现本地获得的病例时促进快速传播控制措施。
本报告总结了 2018 年发病的疟疾病例和前几年的趋势。
通过电子实验室报告或通过医疗保健提供者或实验室工作人员直接向 CDC 或卫生部门报告,通过血涂片显微镜检查、聚合酶链反应或快速诊断检测诊断的疟疾病例报告给当地和州卫生部门。当地和州卫生部门进行病例调查,并通过国家疟疾监测系统(NMSS)、国家法定传染病监测系统(NNDSS)或直接通过 CDC 临床咨询向 CDC 传输报告。CDC 参考实验室提供诊断协助,并对卫生保健提供者或当地或州卫生部门提交的血液标本进行抗疟药物耐药性标志物检测。本报告总结了来自 NMSS 和 NNDSS 的所有病例、CDC 临床咨询和 CDC 参考实验室报告的整合数据。
CDC 收到了 2018 年 1823 例确诊疟疾病例的报告,包括 1 例隐匿性病例和 1 例骨髓移植病例。2018 年报告的病例数比 2017 年减少了 15.6%。自 20 世纪 70 年代中期以来,美国及其领土上的疟疾病例数量一直在增加;2017 年报告的病例数是自 1972 年以来最高的。在 2018 年的病例中,共有 1519 例(85.0%)为源自非洲的输入性病例;来自非洲的病例中,69.9%来自西非,与 2017 年的比例相似。在所有病例中,间日疟原虫感染占大多数(1273 例[69.8%]),其次是卵形疟原虫(173 例[9.5%])、卵形疟原虫(95 例[5.2%])和疟原虫(48 例[2.6%])。自 2008 年以来,首次在美国及其领土上发现输入性疟原虫。两种或两种以上物种的感染占 17 例(<1.0%)。在 216 例病例中(11.9%)未报告或无法确定感染的物种,或未确定感染的物种。大多数(92.6%)患者在从疟疾传播国家返回美国或其领土后 90 天内出现症状。在报告旅行原因的美国平民患者中,77.0%是探亲访友。前往疟疾流行地区旅行的美国居民应服用抗疟药物进行化学预防,以预防疟疾。2018 年,报告服用任何疟疾化学预防药物的美国居民较少(24.5%),低于 2017 年(28.4%),且服用预防药物的人依从性较差。在已知疟疾化学预防药物使用和旅行地区信息的 864 名美国居民中,95.0%的人不符合或未服用 CDC 推荐的化学预防方案。在 683 名疟疾病例女性中,有 19 人报告怀孕。其中,11 名孕妇为美国居民,其中 1 名报告服用化学预防药物预防疟疾,但她的药物依从性未报告。2018 年有 38 例(2.1%)疟疾发生在美国军人中,高于 2017 年(26 例[1.2%])。2018 年,报告的所有疟疾病例中,共有 251 例(13.8%)被归类为严重疟疾,有 7 人死于疟疾。2018 年,CDC 分析了 106 份疟原虫阳性和 4 份疟原虫混合物种标本中的抗疟药物耐药性标志物(尽管某些部位在某些标本中无法检测);发现 99.0%(99 份)存在与抗疟药物嘧啶耐药相关的遗传多态性,49.6%(49 份)存在与磺胺多辛耐药相关的遗传多态性,45.5%(50 份)存在与氯喹耐药相关的遗传多态性,2.0%(2 份)存在与甲氟喹耐药相关的遗传多态性;没有标本检测出对阿托喹酮或青蒿素耐药的标志物。
疟疾的输入反映了与疟疾流行地区的全球旅行的总体趋势,与 2017 年相比,2018 年输入性疟疾病例减少了 15.6%。输入性病例中,59.3%来自西非。在美籍平民中,探亲访友是旅行的最常见原因(77.1%)。
美国居民预防疟疾的最佳方法是在前往疟疾流行地区之前、期间和之后服用化学预防药物。旅行者对推荐的疟疾预防策略的依从性将减少输入性病例的数量。报告的不依从原因包括离开疟疾流行地区后过早停止、忘记服用药物以及出现副作用。卫生保健提供者可以使旅行者意识到疟疾的风险,并纳入教育以促使他们坚持化学预防。如果不及时诊断和治疗,疟疾感染可能致命,使用适当的抗疟药物治疗患者的年龄、妊娠状态、病史、可能获得疟疾的国家以及之前使用的抗疟药物化学预防。抗疟药物的使用,包括化学预防和治疗,应根据 CDC 指南确定,该指南经常更新。2019 年 4 月,静脉(IV)青蒿琥酯成为美国及其领土上治疗疟疾的一线药物。2020 年,青蒿琥酯经食品和药物管理局(FDA)批准,并可从美国主要药品分销商处购买(青蒿琥酯注射液)(https://amivas.com)。当地库存 IV 青蒿琥酯可在确诊后立即进行严重疟疾的治疗,并为患者提供完全康复和无后遗症的最佳机会。随着商业 IV 青蒿琥酯的供应,CDC 将在 2022 年 9 月 30 日停止根据调查性新药协议分发非 FDA 批准的 IV 青蒿琥酯。预防疟疾的详细建议可在 https://www.cdc.gov/malaria/travelers/drugs.html 上获得。疟疾的诊断和治疗建议也可在 https://www.cdc.gov/malaria/diagnosis_treatment 上获得。寻求紧急传染病咨询并需要更多关于疟疾诊断和治疗的帮助的卫生保健提供者可以在东部时间周一至周五上午 9 点至下午 5 点拨打疟疾热线 770-488-7788 或 855-856-4713,或在下午 5 点后拨打紧急查询热线 770-488-7100。报告疟疾病例的卫生保健提供者(提供者、实验室和州和地方公共卫生官员)应提供完整信息,因为不完整的报告会影响病例调查和预防未来感染的公共卫生努力,并检查疟疾病例的趋势。抗疟药物耐药性标志物的分子监测使 CDC 能够跟踪、指导治疗,并在国内外管理疟原虫的耐药性。需要更多的国内疟疾病例标本进行抗疟药物耐药性分析,以提高分析的完整性;因此,CDC 要求从美国和其领土内诊断出的所有疟疾病例中提交血液标本。