Department of Pediatrics, Haukeland University Hospital, Bergen, Norway
Centre for Clinical Research, Haukeland University Hospital, Bergen, Norway.
BMJ Paediatr Open. 2022 Jul;6(1). doi: 10.1136/bmjpo-2022-001527.
To compare outcome after less invasive surfactant administration (LISA) and primary endotracheal intubation (non-LISA) in infants born before gestational age (GA) 28 weeks.
All neonatal intensive care units (NICUs) in Norway during 2012-2018.
Defined population-based data were prospectively entered into a national registry. We compared LISA infants with all non-LISA infants and with non-LISA infants who received surfactant following intubation. We used propensity score (PS) matching to identify non-LISA infants who were similar regarding potential confounders.
Rate and duration of mechanical ventilation (MV), survival, neurological and gastrointestinal morbidity, and need of supplemental oxygen or positive pressure respiratory support at postmenstrual age (PMA) 36 and 40 weeks.
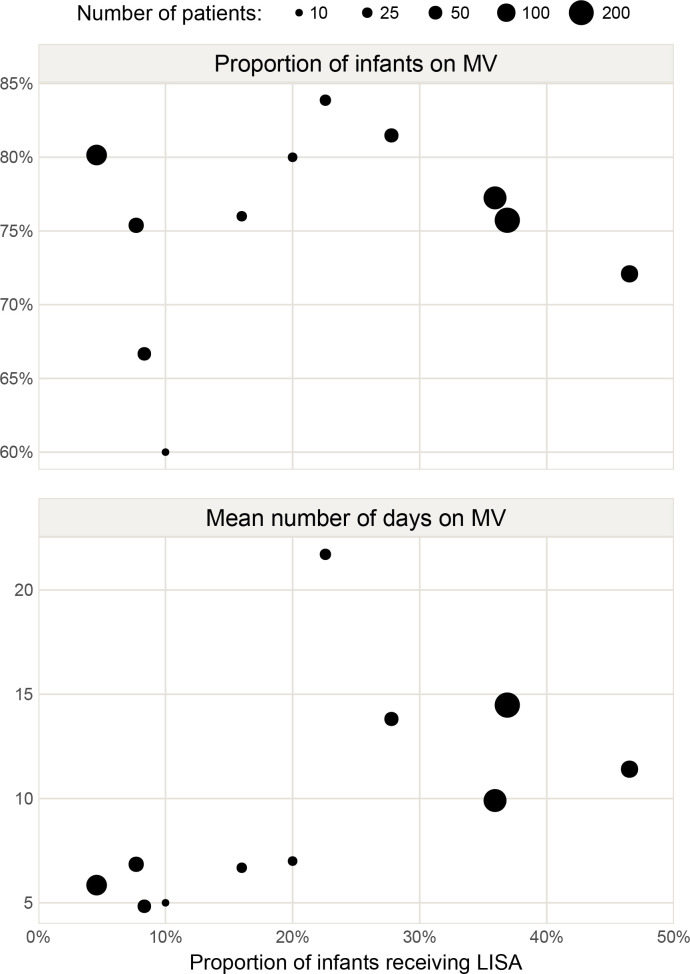
We restricted analyses to GA 25-27 weeks (n=843, 26% LISA) because LISA was rarely used at lower GAs. There was no significant association between NICUs regarding proportions treated with LISA and proportions receiving MV. In the PS-matched datasets, fewer LISA infants received MV (61% vs 78%, p<0.001), and they had fewer days on MV (mean difference 4.1, 95% CI 0.0 to 8.2 days) and lower mortality at PMA 40 weeks (absolute difference 6%, p=0.06) compared with all the non-LISA infants, but only a lower rate of MV (64% vs 97%, p<0.001) and fewer days on MV (mean difference 5.8, 95% CI 0.6 to 10.9 days) compared with non-LISA infants who received surfactant after intubation.
LISA reduced the rate and duration of MV but had no other clear benefits.
比较胎龄(GA)<28 周的婴儿进行微创表面活性剂给药(LISA)和初次气管内插管(非-LISA)后的结局。
2012 年至 2018 年期间挪威所有新生儿重症监护病房(NICU)。
前瞻性地将定义人群的基础数据输入国家登记处。我们将 LISA 婴儿与所有非-LISA 婴儿以及接受插管后表面活性剂治疗的非-LISA 婴儿进行比较。我们使用倾向评分(PS)匹配来识别潜在混杂因素相似的非-LISA 婴儿。
机械通气(MV)的发生率和持续时间、存活率、神经和胃肠道发病率,以及胎龄(PMA)36 和 40 周时补充氧气或正压呼吸支持的需要。
我们将分析限制在 GA 25-27 周(n=843,26%的 LISA),因为 LISA 在较低的 GA 很少使用。NICU 之间关于 LISA 治疗比例和 MV 接受比例没有显著差异。在 PS 匹配的数据集,接受 LISA 的婴儿接受 MV 的比例较低(61%比 78%,p<0.001),接受 MV 的天数也较少(平均差异 4.1,95%CI 0.0 至 8.2 天),并且在 PMA 40 周时死亡率较低(绝对差异 6%,p=0.06),与所有非-LISA 婴儿相比,但仅 MV 率较低(64%比 97%,p<0.001)和 MV 天数较少(平均差异 5.8,95%CI 0.6 至 10.9 天),与插管后接受表面活性剂治疗的非-LISA 婴儿相比。
LISA 降低了 MV 的发生率和持续时间,但没有其他明显的益处。