Department of Cardiovascular and Thoracic Sciences, Catholic University of the Sacred Heart, Rome, Italy.
Department of Translational and Precision Medicine, Sapienza University of Rome, Rome, Italy.
Eur J Heart Fail. 2022 Dec;24(12):2333-2341. doi: 10.1002/ejhf.2655. Epub 2022 Sep 11.
Pre-clinical congestion markers of worsening heart failure (HF) can be monitored by devices and may support the management of patients with HF. We aimed to assess whether congestion-guided HF management according to device-based remote monitoring strategies is more effective than standard therapy.
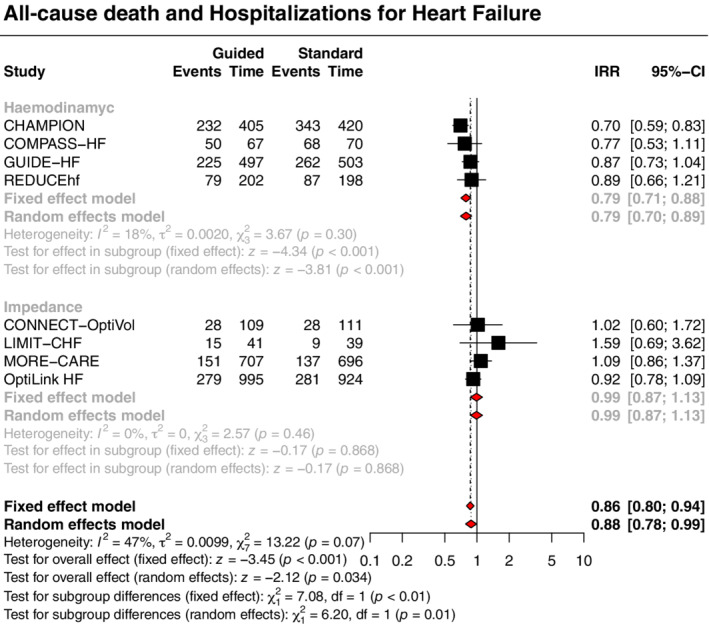
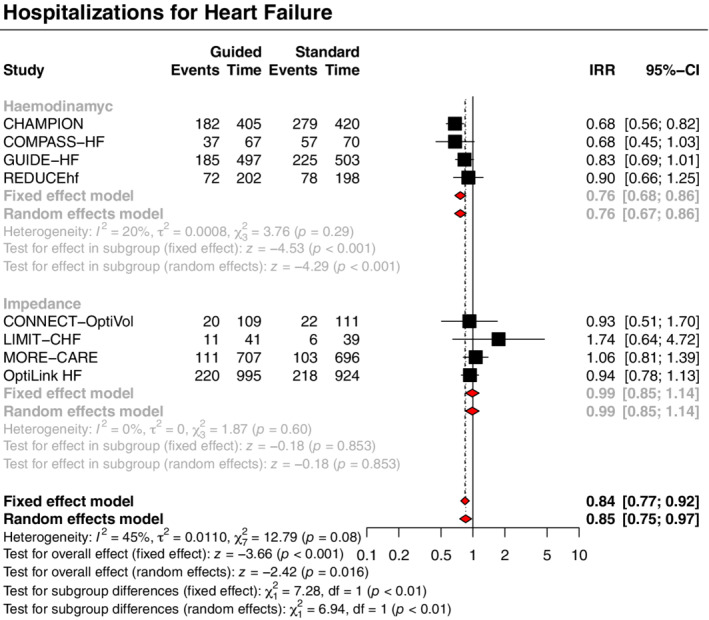
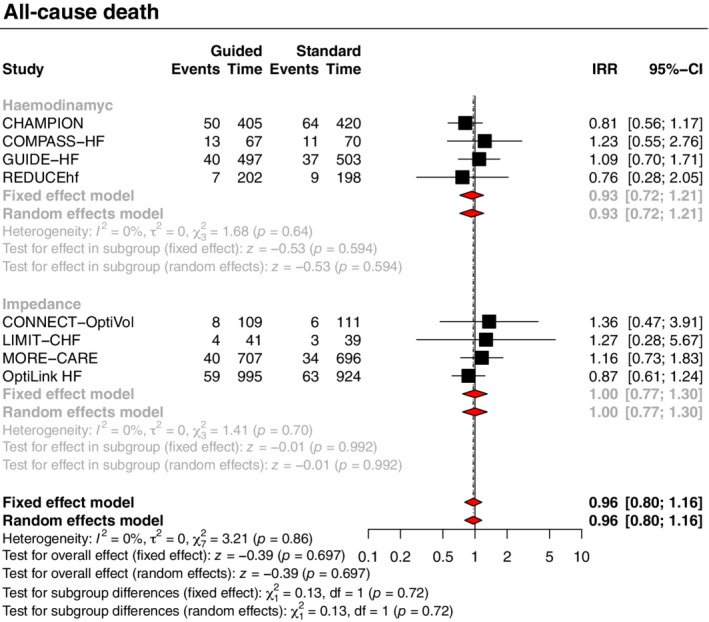
A comprehensive literature research for randomized controlled trials (RCTs) comparing device-based remote monitoring strategies for congestion-guided HF management versus standard therapy was performed on PubMed, Embase, and CENTRAL databases. Incidence rate ratios (IRRs) and associated 95% confidence intervals (CIs) were calculated using the Poisson regression model with random study effects. The primary outcome was a composite of all-cause death and HF hospitalizations. Secondary endpoints included the individual components of the primary outcome. A total of 4347 patients from eight RCTs were included. Findings varied according to the type of parameters monitored. Compared with standard therapy, haemodynamic-guided strategy (4 trials, 2224 patients, 12-month follow-up) reduced the risk of the primary composite outcome (IRR 0.79, 95% CI 0.70-0.89) and HF hospitalizations (IRR 0.76, 95% CI 0.67-0.86), without a significant impact on all-cause death (IRR 0.93, 95% CI 0.72-1.21). In contrast, impedance-guided strategy (4 trials, 2123 patients, 19-month follow-up) did not provide significant benefits.
Haemodynamic-guided HF management is associated with better clinical outcomes as compared to standard clinical care.
可以通过设备监测到恶化心力衰竭(HF)的临床前充血标志物,这可能有助于 HF 患者的管理。我们旨在评估基于设备的远程监测策略指导充血的 HF 管理是否比标准治疗更有效。
在 PubMed、Embase 和 CENTRAL 数据库中进行了全面的文献检索,以评估比较基于设备的远程监测策略指导充血的 HF 管理与标准治疗的随机对照试验(RCT)。使用具有随机研究效应的泊松回归模型计算发生率比(IRR)和相关的 95%置信区间(CI)。主要结局是全因死亡和 HF 住院的复合结局。次要终点包括主要结局的各个组成部分。共纳入了来自 8 项 RCT 的 4347 名患者。研究结果因监测参数的类型而异。与标准治疗相比,血流动力学指导策略(4 项试验,2224 名患者,12 个月随访)降低了主要复合结局的风险(IRR 0.79,95%CI 0.70-0.89)和 HF 住院(IRR 0.76,95%CI 0.67-0.86),但对全因死亡无显著影响(IRR 0.93,95%CI 0.72-1.21)。相比之下,阻抗指导策略(4 项试验,2123 名患者,19 个月随访)并未提供显著益处。
与标准临床护理相比,血流动力学指导的 HF 管理与更好的临床结局相关。