Department of Thoracic Surgery, Fujian Medical University Union Hospital, Fuzhou, P. R. China.
Department of Thoracic Surgery, Xiamen Humanity Hospital of Fujian Medical University, Xiamen, P. R. China.
Thorac Cancer. 2022 Oct;13(20):2879-2889. doi: 10.1111/1759-7714.14633. Epub 2022 Sep 4.
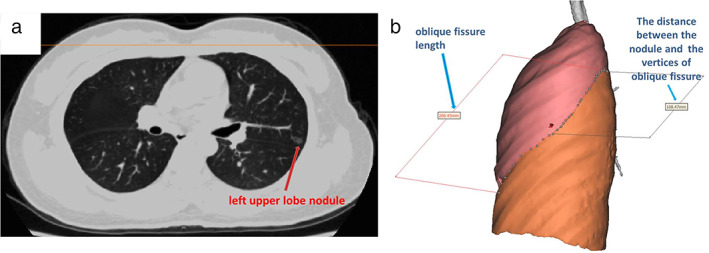
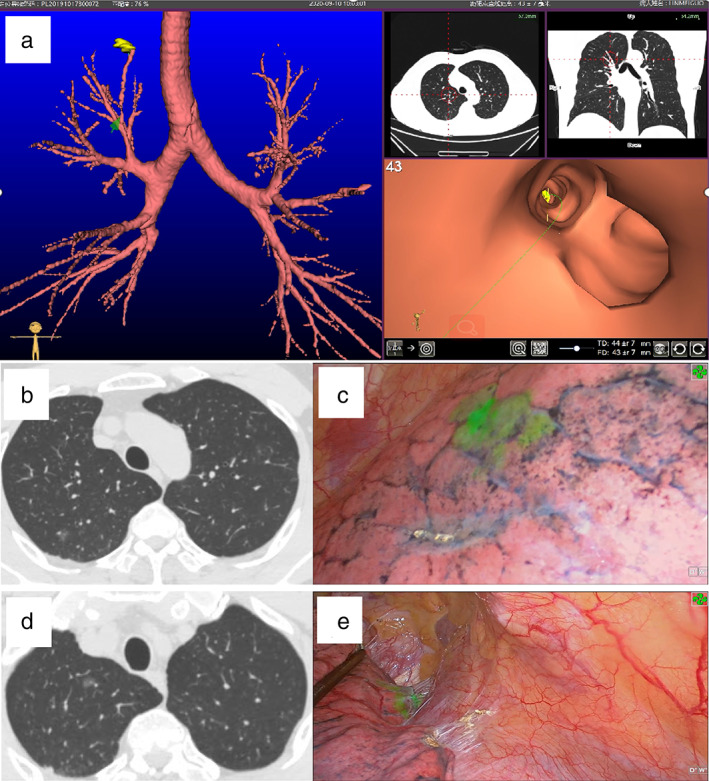
Accurate localization of pulmonary nodules is the main difficulty experienced in wedge resection. Commonly used localization methods have their own advantages and disadvantages. However, clinical work has demonstrated that intraoperative indocyanine green localization under electromagnetic navigation bronchoscopy/virtual navigation bronchoscopy (VNB) is more advantageous than conventional methods for patients with multiple pulmonary nodules undergoing simultaneous surgery, especially for those undergoing bilateral lung surgery.
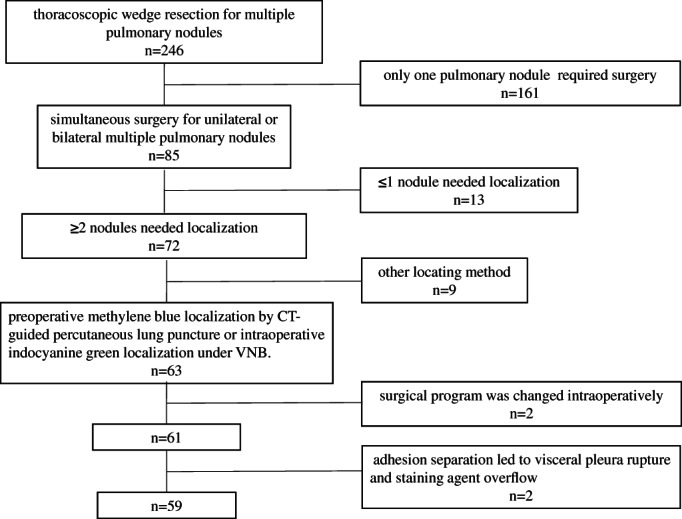
Data of patients undergoing simultaneous surgery for multiple pulmonary nodules with preoperative methylene blue localization by computed tomography (CT)-guided percutaneous lung puncture (methylene blue group) or intraoperative indocyanine green localization under VNB (virtual navigation group) were retrospectively analyzed. Patient characteristics, pulmonary nodule features, localization time, preoperative location time, location success rate, operation time, complication incidence, visceral pleural staining rate after localization, and pulmonary nodule primary resection success rate were compared between the two groups.
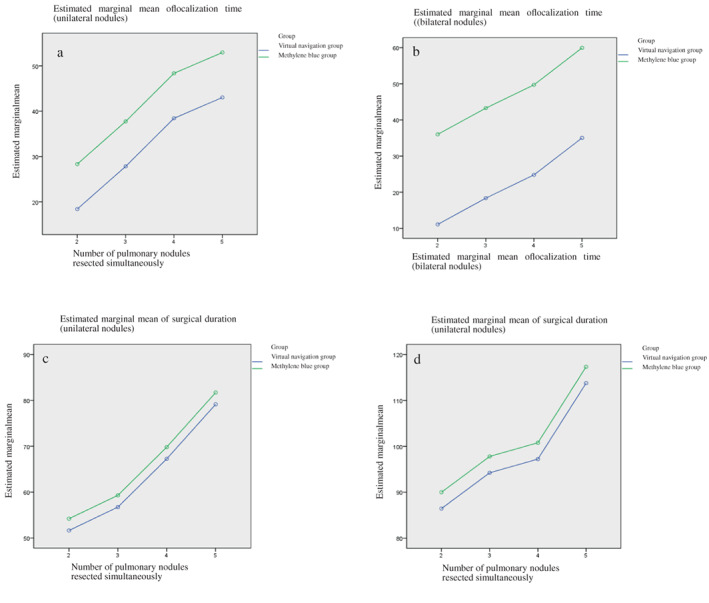
The methylene blue and virtual navigation groups comprised 39 and 20 patients with 119 and 67 pulmonary nodules resected, respectively. Sex, age, number of pulmonary nodules resected simultaneously, unilateral/bilateral lung surgery, pulmonary nodule size, distance between pulmonary nodules and the visceral pleura, pulmonary nodule consolidation-to-tumor ratio, location of pulmonary nodules in the pulmonary lobe, postoperative pathology, visceral pleura staining rate, primary pulmonary nodule resection success rate, and surgical duration did not differ significantly between the groups (p > 0.05). The localization time of the virtual navigation group was significantly shorter than that of the methylene blue group (p < 0.05), regardless of unilateral or bilateral multiple nodules. In the methylene blue group, 25.64% (10/39) of patients presented complications, all of which were pneumothorax, whereas no complications were found in the virtual navigation group.
For patients with multiple pulmonary nodules undergoing simultaneous surgery, indocyanine green injection under VNB can achieve a similar effect on pulmonary nodule localization as classical methylene blue injection under CT-guided percutaneous lung puncture, with shorter localization time and fewer complications.
肺结节的准确定位是楔形切除术中遇到的主要难点。常用的定位方法各有优缺点。但临床工作中发现,电磁导航支气管镜/虚拟导航支气管镜(VNB)下术中吲哚菁绿定位对于同时行多肺结节手术的患者,尤其是双侧肺手术患者,较传统方法更具优势。
回顾性分析术前 CT 引导下经皮肺穿刺行亚甲蓝定位(亚甲蓝组)或 VNB 下术中吲哚菁绿定位(虚拟导航组)行多肺结节同期手术患者的资料。比较两组患者的一般资料、肺结节特征、定位时间、术前定位时间、定位成功率、手术时间、并发症发生率、定位后脏层胸膜染色率、肺结节原发病灶切除成功率。
亚甲蓝组和虚拟导航组分别纳入 39 例和 20 例患者,共切除 119 个和 67 个肺结节。两组患者的性别、年龄、同期切除肺结节数、单侧/双侧肺手术、肺结节大小、肺结节与脏层胸膜的距离、肺结节实变/肿瘤比值、肺结节所在肺叶、术后病理、脏层胸膜染色率、肺结节原发病灶切除成功率、手术时间差异均无统计学意义(p>0.05)。无论单侧或双侧多发肺结节,虚拟导航组的定位时间均显著短于亚甲蓝组(p<0.05)。亚甲蓝组中,25.64%(10/39)的患者出现并发症,均为气胸,而虚拟导航组无并发症发生。
对于多肺结节同期手术患者,VNB 下注射吲哚菁绿行肺结节定位与 CT 引导下经皮肺穿刺亚甲蓝注射定位效果相当,但定位时间更短、并发症更少。