Shantou Central Hospital, Shantou, China.
Guangdong Provincial People's Hospital & Guangdong Academy of Medical Sciences, Guangzhou, China.
Thorac Cancer. 2021 Feb;12(4):468-474. doi: 10.1111/1759-7714.13775. Epub 2021 Jan 4.
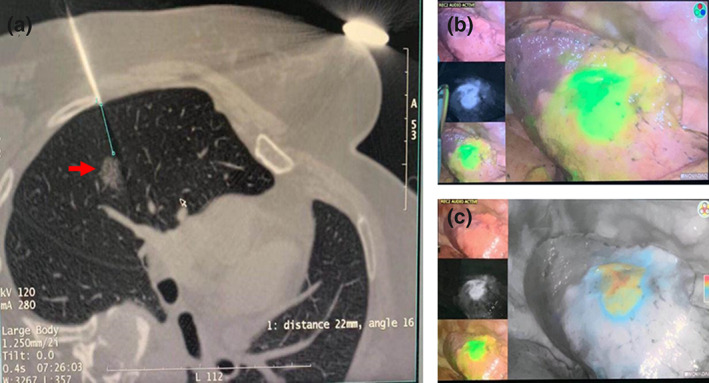
Identification of small pulmonary nodules is challenging in a limited intrathoracic field during minimally invasive video-assisted thoracoscopic surgery (VATS), and preoperative localization is required. Various techniques have been reported with some failure and complications. Here, we compare the feasibility and safety between electromagnetic navigation bronchoscopic marking and computed tomography (CT)-guided percutaneous marking using indocyanine green (ICG) and iopamidol.
A total of 47 patients with small-sized pulmonary nodules, scheduled to undergo video-assisted thoracoscopic limited resection, were enrolled in this study. A mixture of diluted ICG and iopamidol was injected into the lung parenchyma as a marker, using CT-guided percutaneous or electromagnetic navigation bronchoscopic injection techniques and the results were examined and compared.
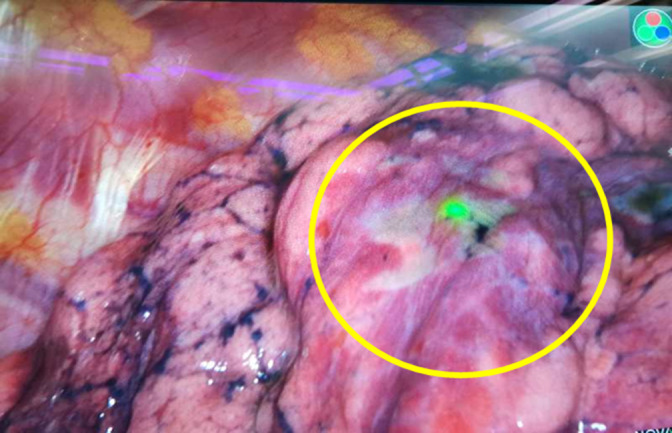
A total of 35 and 12 patients underwent preoperative marking by percutaneous injection and electromagnetic navigation bronchoscopic injection, respectively, in which a marker was detected in 33/35 (94.3%) and 12/12 (100%) patients. No combination of these procedures was performed in any patient. All markers were successfully detected in three patients who underwent injection marking at two different lesion sites. Pneumothorax occurred in five patients (14%) in the percutaneous marking group, which was relieved in all patients without the necessity for chest tube drainage. No other complication was observed in this study.
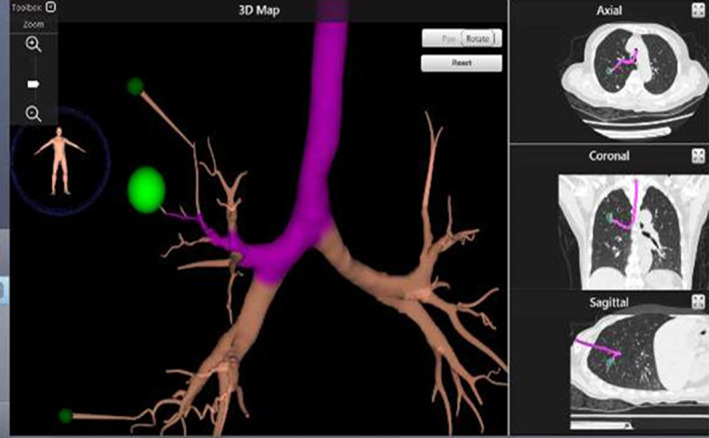
Electromagnetic navigation bronchoscopic injection techniques using indocyanine green fluorescence plus iopamidol are safe and effective, and comparable with CT-guided localization. Furthermore, a bronchoscopic approach enables marking of multiple lesion areas without increasing patient risk, especially for puncture-related pneumothorax.
SIGNIFICANT FINDINGS OF THE STUDY: Either computed tomography (CT)-guided percutaneous or electromagnetic navigation bronchoscopic injection techniques can be used for preoperative marking of pulmonary nodules with indocyanine green (ICG) fluorescence.
Indocyanine green (ICG) is a safe and easily detectable fluorescent marker for video-assisted thoracoscopic surgery (VATS). A bronchoscopic injection approach enables marking of multiple lesion areas without increasing the risk of pneumothorax.
在微创电视辅助胸腔镜手术(VATS)中,有限的胸腔内区域内难以识别小的肺结节,需要进行术前定位。已经报道了各种技术,但有些技术存在失败和并发症。在这里,我们比较了电磁导航支气管镜标记和 CT 引导经皮标记使用吲哚菁绿(ICG)和碘帕醇的可行性和安全性。
本研究共纳入 47 例拟行电视辅助胸腔镜下局限性肺切除术的小肺结节患者。将稀释后的 ICG 和碘帕醇混合物作为标记物注入肺实质,采用 CT 引导经皮或电磁导航支气管镜注射技术,并对结果进行检查和比较。
共有 35 例和 12 例患者分别接受经皮注射和电磁导航支气管镜注射术前标记,33/35(94.3%)和 12/12(100%)患者中检测到标记物。没有患者同时进行这些操作的组合。在三个在两个不同病变部位进行注射标记的患者中,所有标记物均成功检测到。在经皮标记组中,5 例(14%)患者发生气胸,所有患者均自行缓解,无需胸腔引流。本研究未观察到其他并发症。
使用吲哚菁绿荧光加碘帕醇的电磁导航支气管镜注射技术安全有效,与 CT 引导定位相当。此外,支气管镜方法可标记多个病变部位,而不会增加患者的风险,尤其是对于与穿刺相关的气胸。