Department of Surgery, Máxima Medical Center, Veldhoven, The Netherlands.
University of Amsterdam, Amsterdam, The Netherlands.
BMC Surg. 2022 Sep 4;22(1):330. doi: 10.1186/s12893-022-01765-y.
Adequate pain control after video-assisted thoracoscopic surgery (VATS) for lung resection is important to improve postoperative mobilisation, recovery, and to prevent pulmonary complications. So far, no consensus exists on optimal postoperative pain management after VATS anatomic lung resection. Thoracic epidural analgesia (TEA) is the reference standard for postoperative pain management following VATS. Although the analgesic effect of TEA is clear, it is associated with patient immobilisation, bladder dysfunction and hypotension which may result in delayed recovery and longer hospitalisation. These disadvantages of TEA initiated the development of unilateral regional techniques for pain management. The most frequently used techniques are continuous paravertebral block (PVB) and single-shot intercostal nerve block (ICNB). We hypothesize that using either PVB or ICNB is non-inferior to TEA regarding postoperative pain and superior regarding quality of recovery (QoR). Signifying faster postoperative mobilisation, reduced morbidity and shorter hospitalisation, these techniques may therefore reduce health care costs and improve patient satisfaction.
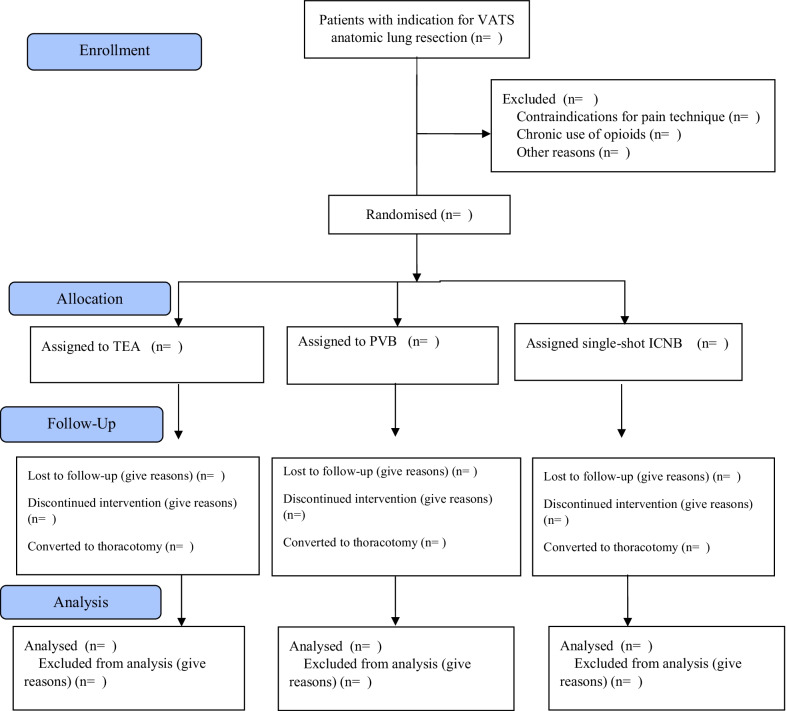
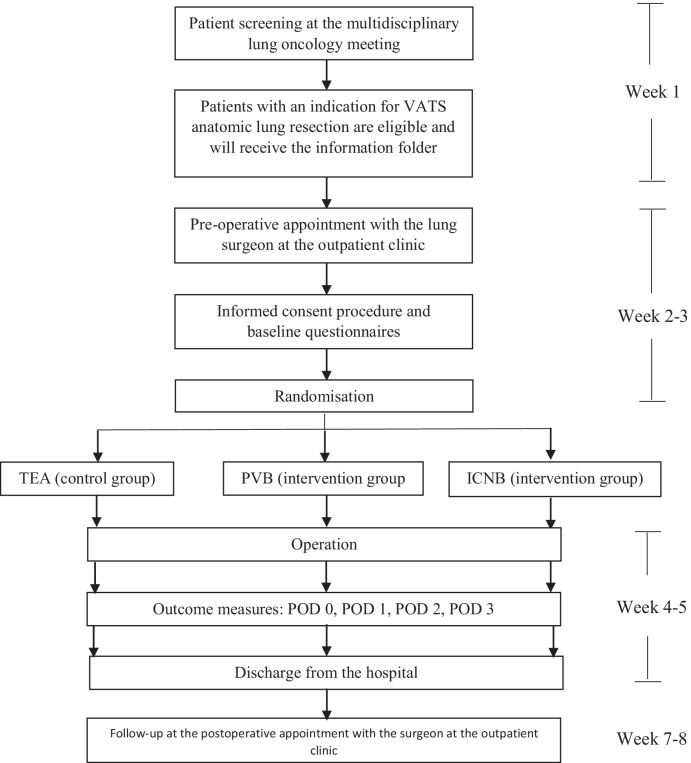
This multi-centre randomised study is a three-arm clinical trial comparing PVB, ICNB and TEA in a 1:1:1 ratio for pain (non-inferiority) and QoR (superiority) in 450 adult patients undergoing VATS anatomic lung resection. Patients will not be eligible for inclusion in case of contraindications for TEA, PVB or ICNB, chronic opioid use or if the lung surgeon estimates a high probability that the operation will be performed by thoracotomy.
(1) the proportion of pain scores ≥ 4 as assessed by the numerical rating scale (NRS) measured during postoperative days (POD) 0-2; and (2) the QoR measured with the QoR-15 questionnaire on POD 1 and 2. Secondary outcome measures are cumulative use of opioids and analgesics, postoperative complications, hospitalisation, patient satisfaction and degree of mobility.
The results of this trial will impact international guidelines with respect to perioperative care optimization after anatomic lung resection performed through VATS, and will determine the most cost-effective pain strategy and may reduce variability in postoperative pain management. Trial registration The trial is registered at the Netherlands Trial Register (NTR) on February 1st, 2021 (NL9243). The NTR is no longer available since June 24th, 2022 and therefore a revised protocol has been registered at ClinicalTrials.gov on August 5th, 2022 (NCT05491239).
version 3 (date 06-05-2022), ethical approval through an amendment (see ethical proof in the Study protocol proof).
视频辅助胸腔镜手术(VATS)后充分的疼痛控制对于改善术后活动能力、恢复和预防肺部并发症非常重要。到目前为止,对于 VATS 解剖性肺切除术后的最佳术后疼痛管理还没有共识。胸椎硬膜外镇痛(TEA)是 VATS 后术后疼痛管理的参考标准。尽管 TEA 的镇痛效果明确,但它与患者的固定、膀胱功能障碍和低血压有关,这可能导致恢复延迟和住院时间延长。TEA 的这些缺点促使人们开发了用于疼痛管理的单侧区域技术。最常使用的技术是连续椎旁阻滞(PVB)和单次肋间神经阻滞(ICNB)。我们假设,在术后疼痛方面,使用 PVB 或 ICNB 与 TEA 相比不劣,在恢复质量(QoR)方面具有优势。这些技术可促进术后更快地活动、降低发病率和缩短住院时间,因此可能会降低医疗保健成本并提高患者满意度。
这是一项多中心随机研究,是一项三臂临床试验,将 450 名接受 VATS 解剖性肺切除术的成年患者以 1:1:1 的比例随机分为 PVB、ICNB 和 TEA 三组,比较三组在疼痛(非劣效性)和 QoR(优效性)方面的差异。如果存在 TEA、PVB 或 ICNB 的禁忌证、慢性阿片类药物使用或肺外科医生估计手术很可能通过开胸进行,则患者将没有资格入组。
(1)术后第 0-2 天通过数字评分量表(NRS)测量的疼痛评分≥4的比例;(2)术后第 1 天和第 2 天用 QoR-15 问卷测量的 QoR。次要结局指标为累积使用阿片类药物和镇痛药、术后并发症、住院时间、患者满意度和活动度。
该试验的结果将影响国际指南中关于通过 VATS 进行解剖性肺切除术后围手术期护理的优化,并将确定最具成本效益的疼痛策略,并可能减少术后疼痛管理的变异性。试验注册该试验于 2021 年 2 月 1 日在荷兰试验注册处(NTR)注册(NL9243)。自 2022 年 6 月 24 日起,NTR 不再可用,因此于 2022 年 8 月 5 日在 ClinicalTrials.gov 上注册了修订后的方案(NCT05491239)。
第 3 版(日期 2022 年 6 月 5 日),通过修正案获得伦理批准(请在研究方案证明中查看伦理证明)。