Zhang Ting, Feng Hua, Xiao Wei, Li Jingsheng, Liu Qinghai, Feng Xuexin, Qi Dezhou, Fan Xiaotong, Shan Yongzhi, Yu Tao, Zhao Guoguang, Wang Tianlong
Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, Beijing, China.
Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China.
Front Pharmacol. 2022 Aug 17;13:916017. doi: 10.3389/fphar.2022.916017. eCollection 2022.
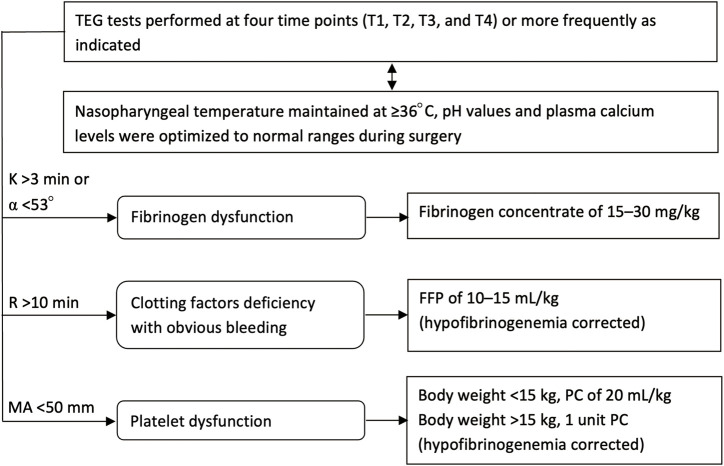
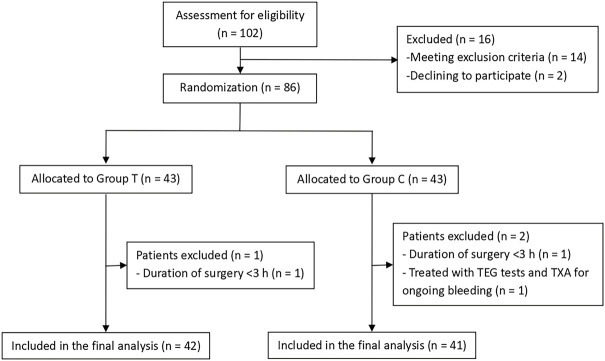
Intraoperative bleeding and allogeneic transfusion remain common problems in pediatric resective epilepsy surgery. Tranexamic acid (TXA) is a widely recommended antifibrinolytic drug that reduces blood loss and transfusion requirements for bleeding patients. Thromboelastography (TEG)-guided hemostatic algorithm is commonly used in bleeding management. This trial was designed to validate the efficacy of a multimodal coagulation therapy involving continuous TXA infusion with TEG-guided hemostatic algorithm in reducing allogeneic exposure risk in pediatric resective epilepsy surgery. Eighty-three children undergoing resective epilepsy surgery were randomized into a treatment group (Group T; = 42) and a control group (Group C; = 41). Group T received prophylactic TXA (10 mg/kg followed by 5 mg/kg/h) with TEG-guided hemostatic algorithm, whereas Group C received conventional coagulation management. The primary outcome was allogeneic transfusion rate during surgery, and the secondary outcomes were intraoperative blood loss, incidence of postoperative seizures, and thromboembolic events during hospitalization. The incidence of intraoperative allogeneic transfusion reduced by 34.7% with the use of a multimodal coagulation therapy (19.0% in Group T vs. 53.7% in Group C; RR 0.355, 95% CI 0.179-0.704; = 0.001). This was mainly triggered by a significant reduction (44.1%) in intraoperative plasma transfusion (7.1% in Group T vs. 51.2% in Group C; RR 0.139, 95% CI 0.045-0.432; = 0.000). The risk of intraoperative RBC transfusion was lower in Group T than in Group C, but the difference was not statistically significant (14.3% in Group T vs. 29.3% in Group C; RR 0.488, 95% CI 0.202-1.177; = 0.098). No platelets were transfused in both groups. Further, 19 (45.2%) patients in Group T received fibrinogen concentrates guided by TEG data, whereas 1 (2.4%) patient in Group C received fibrinogen concentrates empirically. There were no significant differences in estimated blood loss and postoperative seizures between the two groups, and no thromboembolic events were observed after surgery. Prophylactic administration of TXA combined with TEG-guided hemostatic algorithm can be an effective multimodal coagulation strategy for reducing allogeneic transfusion requirements during pediatric resective epilepsy surgery. www.chictr.org.cn/index.aspx, identifier ChiCTR1800016188.
术中出血和异体输血仍是小儿切除性癫痫手术中常见的问题。氨甲环酸(TXA)是一种广泛推荐的抗纤溶药物,可减少出血患者的失血量和输血需求。血栓弹力图(TEG)引导的止血算法常用于出血管理。本试验旨在验证一种多模式凝血疗法的疗效,该疗法包括持续输注TXA并结合TEG引导的止血算法,以降低小儿切除性癫痫手术中异体输血的风险。83例接受切除性癫痫手术的儿童被随机分为治疗组(T组;n = 42)和对照组(C组;n = 41)。T组接受预防性TXA(10 mg/kg,随后5 mg/kg/h)并采用TEG引导的止血算法,而C组接受传统的凝血管理。主要结局是手术期间的异体输血率,次要结局是术中失血量、术后癫痫发作的发生率以及住院期间的血栓栓塞事件。使用多模式凝血疗法后,术中异体输血的发生率降低了34.7%(T组为19.0%,C组为53.7%;RR 0.355,95%CI 0.179 - 0.704;P = 0.001)。这主要是由于术中血浆输注显著减少(44.1%)(T组为7.1%,C组为51.2%;RR 0.139,95%CI 0.045 - 0.432;P = 0.000)。T组术中红细胞输血的风险低于C组,但差异无统计学意义(T组为14.3%,C组为29.3%;RR 0.488,95%CI 0.202 - 1.177;P = 0.098)。两组均未输注血小板。此外,T组有19例(45.2%)患者根据TEG数据接受了纤维蛋白原浓缩剂,而C组有1例(2.4%)患者经验性地接受了纤维蛋白原浓缩剂。两组之间的估计失血量和术后癫痫发作无显著差异,术后未观察到血栓栓塞事件。预防性给予TXA并结合TEG引导的止血算法可能是一种有效的多模式凝血策略,可减少小儿切除性癫痫手术期间的异体输血需求。www.chictr.org.cn/index.aspx,标识符ChiCTR1800016188 。