Cancer Health Services Research, Centre for Cancer Research, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Melbourne, Australia.
Sir Peter MacCallum Department of Oncology, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Melbourne, Australia.
Target Oncol. 2022 Sep;17(5):539-548. doi: 10.1007/s11523-022-00910-0. Epub 2022 Sep 5.
Complex genomic profiling (CGP) has transformed cancer treatment decision making, yet there is a lack of robust and quantifiable evidence for how utilisation of CGP improves patient outcomes.
This study evaluated cohort level clinical effectiveness of CGP to improve overall survival (OS) in real-world advanced cancer patients using a registry-based matched control population.
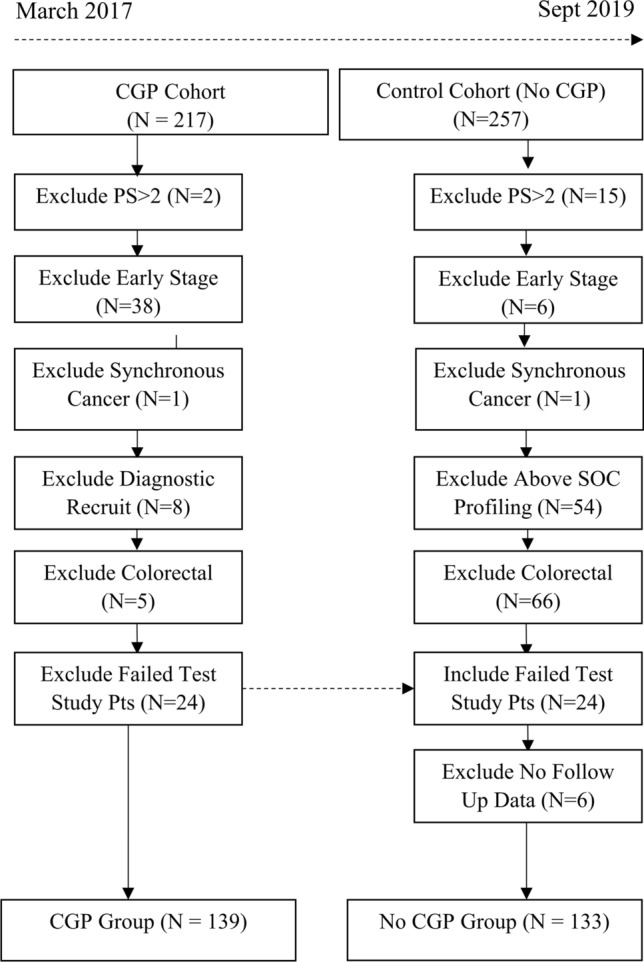
Two cohorts of advanced and refractory cancer patients were seen in consecutive series for early phase trial enrolment consideration. The first cohort (CGP group) accessed tumour profiling via a research study; while the second cohort that followed was not profiled. Overall survival between cohorts was compared using Kaplan-Meier curves and Cox proportional hazard models. Potential confounding was analysed and adjusted for using stabilised weights based on propensity scores.
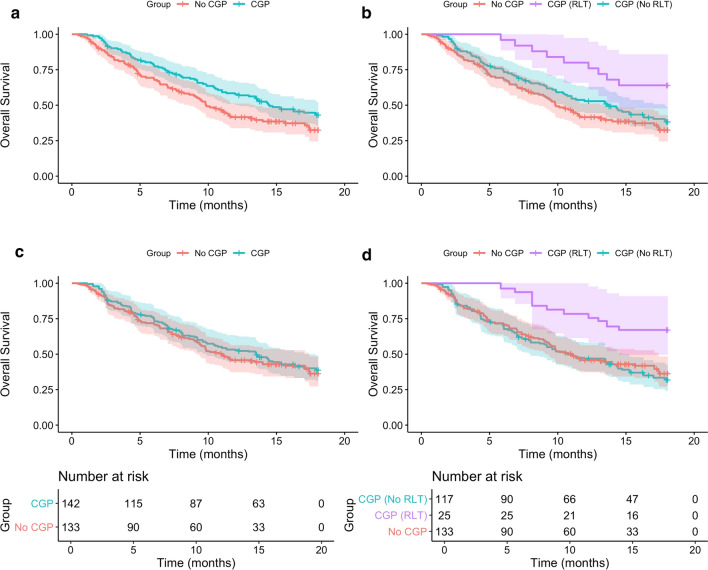
Within the CGP group, 25 (17.6%) patients received treatment informed by CGP results and this subgroup had significantly improved survival compared with CGP patients in whom results did not impact their treatment (unadjusted HR = 0.44, (0.22-0.88), p = 0.02). However, when comparing the entire CGP cohort with the No CGP cohort, no significant survival benefit was evident with adjusted median OS for CGP of 13.5 months (9.2-17.0) compared with 11.0 (9.2-17.4) for No CGP (adjusted HR = 0.92, (0.65-1.30), p = 0.63).
This study utilised real-world data to simulate a control arm and quantify the clinical effectiveness of genomic testing. The magnitude of survival benefit for patients who had CGP result-led treatments was insufficient to drive an overall survival gain for the entire tested population. Translation of CGP into clinics requires strategies to ensure higher rates of tested patients obtain clinical benefit to deliver on the value proposition of CGP in an advanced cancer population.
复杂基因组分析(CGP)改变了癌症治疗决策,但缺乏关于 CGP 如何改善患者预后的有力和可量化的证据。
本研究通过基于登记的匹配对照人群,评估 CGP 在真实世界晚期癌症患者中提高总生存率(OS)的队列水平临床效果。
为早期阶段试验入组考虑,连续系列中观察到两组晚期和难治性癌症患者。第一组(CGP 组)通过研究获得肿瘤分析;而随后的第二组没有进行分析。使用 Kaplan-Meier 曲线和 Cox 比例风险模型比较两组之间的总生存情况。使用基于倾向评分的稳定权重进行潜在混杂因素分析和调整。
在 CGP 组中,25 名(17.6%)患者接受了 CGP 结果指导的治疗,与 CGP 结果未影响其治疗的患者相比,该亚组的生存明显改善(未调整 HR=0.44,(0.22-0.88),p=0.02)。然而,当将整个 CGP 队列与无 CGP 队列进行比较时,调整后的中位 OS 对 CGP 为 13.5 个月(9.2-17.0),而无 CGP 为 11.0 个月(9.2-17.4),无显著生存获益(调整后的 HR=0.92,(0.65-1.30),p=0.63)。
本研究利用真实世界数据模拟对照臂并量化基因组检测的临床效果。接受 CGP 结果指导治疗的患者的生存获益幅度不足以使整个受试人群的总生存率提高。CGP 在临床中的转化需要策略来确保更多接受测试的患者获得临床获益,以实现在晚期癌症人群中 CGP 的价值主张。