Department of Anesthesiology, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, China.
Department of Anesthesiology, Zhongshan People's Hospital, Zhongshan, 528400, Guangdong, China.
Mil Med Res. 2022 Sep 5;9(1):49. doi: 10.1186/s40779-022-00403-1.
Data on severe and extensive burns in China are limited, as is data on the prevalence of a range of related gastrointestinal (GI) disorders [such as stress ulcers, delayed defecation, opioid-related bowel immotility, and abdominal compartment syndrome (ACS)]. We present a multicentre analysis of coincident GI dysfunction and its effect on burn-related mortality.
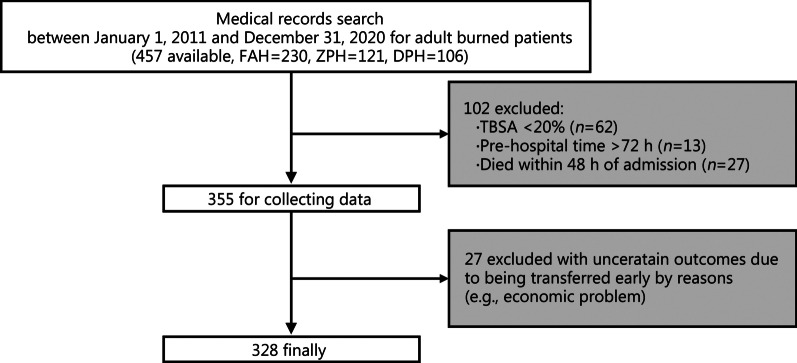
This retrospective analysis was conducted on patients with severe [≥ 20% total burn surface area (TBSA)] and extensive (> 50% TBSA or > 25% full-thickness TBSA) burns admitted to three university teaching institutions in China between January 1, 2011 and December 31, 2020. Both 30- and 90-day mortality were assessed by collating demographic data, burn causes, admission TBSA, % full-thickness TBSA, Baux score, Abbreviated Burn Severity Index (ABSI) score, and Sequential Organ Failure Assessment (SOFA) score, shock at admission and the presence of an inhalation injury. GI dysfunction included abdominal distension, nausea/vomiting, diarrhoea/constipation, GI ulcer/haemorrhage, paralytic ileus, feeding intolerance and ACS. Surgeries, length of intensive care unit (ICU) stay, pain control [in morphine milligram equivalents (MME)] and overall length of hospital stay (LOHS) were recorded.
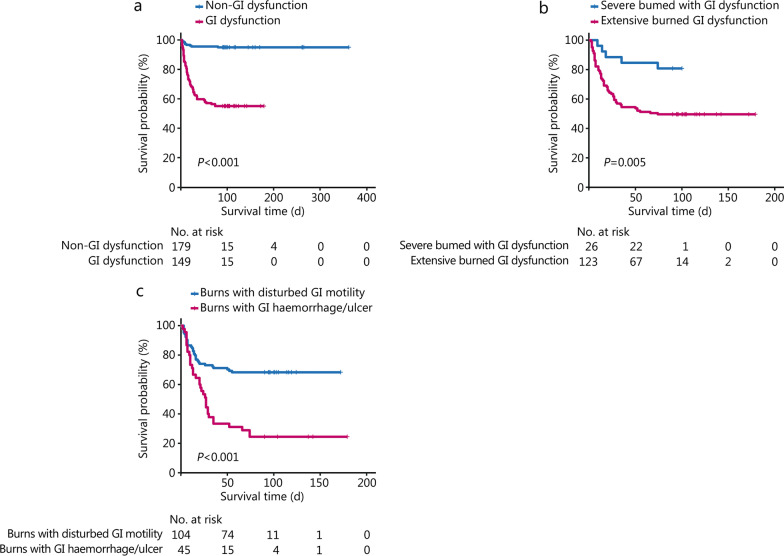
We analyzed 328 patients [75.6% male, mean age: (41.6 ± 13.6) years] with a median TBSA of 62.0% (41.0-80.0%); 256 (78.0%) patients presented with extensive burns. The 90-day mortality was 23.2% (76/328), with 64 (84.2%) of these deaths occurring within 30 d and 25 (32.9%) occurring within 7 d. GI dysfunction was experienced by 45.4% of patients and had a significant effect on 90-day mortality [odds ratio (OR) = 14.070, 95% confidence interval (CI) 5.886-38.290, P < 0.001]. Multivariate analysis showed that GI dysfunction was associated with admission SOFA score and % full-thickness TBSA. Overall, 88.2% (67/76) of deceased patients had GI dysfunction [hazard ratio (HR) for death of GI dysfunction = 5.951], with a survival advantage for functional disorders (diarrhoea, constipation, or nausea/vomiting) over GI ulcer/haemorrhage (P < 0.001).
Patients with severe burns have an unfavourable prognosis, as nearly one-fifth died within 90 d. Half of our patients had comorbidities related to GI dysfunction, among which GI ulcers and haemorrhages were independently correlated with 90-day mortality. More attention should be given to severe burn patients with GI dysfunction.
中国严重和大面积烧伤的数据有限,涉及一系列相关胃肠道(GI)疾病的患病率数据也有限[如应激性溃疡、延迟排便、阿片类药物相关肠道运动障碍和腹腔间隔室综合征(ACS)]。我们报告了一项多中心分析,内容为同时发生的胃肠道功能障碍及其对烧伤相关死亡率的影响。
本回顾性分析纳入了 2011 年 1 月 1 日至 2020 年 12 月 31 日期间在中国三所大学教学机构收治的严重(≥20%总体烧伤表面积(TBSA))和大面积(>50% TBSA 或>25%全厚 TBSA)烧伤患者。通过整理人口统计学数据、烧伤原因、入院 TBSA、%全厚 TBSA、Baux 评分、简化烧伤严重程度指数(ABSI)评分和序贯器官衰竭评估(SOFA)评分、入院时休克和吸入性损伤情况,评估 30 天和 90 天死亡率。胃肠道功能障碍包括腹胀、恶心/呕吐、腹泻/便秘、GI 溃疡/出血、麻痹性肠梗阻、喂养不耐受和 ACS。记录了手术、重症监护病房(ICU)住院时间、疼痛控制(以吗啡毫克当量(MME)表示)和总住院时间(LOHS)。
我们分析了 328 例患者[75.6%为男性,平均年龄:(41.6±13.6)岁],中位 TBSA 为 62.0%(41.0-80.0%);256 例(78.0%)患者为大面积烧伤。90 天死亡率为 23.2%(76/328),其中 64 例(84.2%)死亡发生在 30 天内,25 例(32.9%)发生在 7 天内。45.4%的患者出现胃肠道功能障碍,且与 90 天死亡率显著相关[比值比(OR)=14.070,95%置信区间(CI)5.886-38.290,P<0.001]。多变量分析显示,胃肠道功能障碍与入院 SOFA 评分和%全厚 TBSA 有关。总体而言,76 例死亡患者中有 88.2%(67/76)有胃肠道功能障碍[胃肠道功能障碍死亡的风险比(HR)为 5.951],功能性障碍(腹泻、便秘或恶心/呕吐)的生存优势高于 GI 溃疡/出血(P<0.001)。
严重烧伤患者预后不佳,近五分之一的患者在 90 天内死亡。我们的一半患者存在与胃肠道功能障碍相关的合并症,其中 GI 溃疡和出血与 90 天死亡率独立相关。应更加关注有胃肠道功能障碍的严重烧伤患者。