Escobar Carlos, Palacios Beatriz, Varela Luis, Gutiérrez Martín, Duong Mai, Chen Hungta, Justo Nahila, Cid-Ruzafa Javier, Hernández Ignacio, Hunt Phillip R, Delgado Juan F
Cardiology Department, University Hospital La Paz, 28046 Madrid, Spain.
AstraZeneca Farmaceutica, 28033 Madrid, Spain.
J Clin Med. 2022 Sep 2;11(17):5199. doi: 10.3390/jcm11175199.
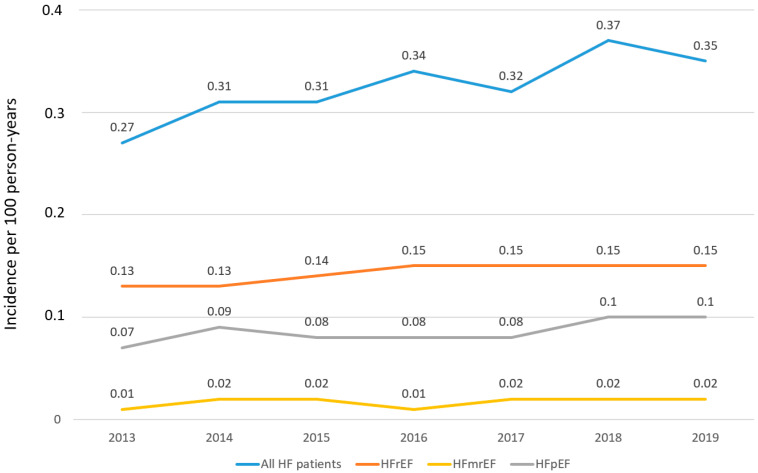
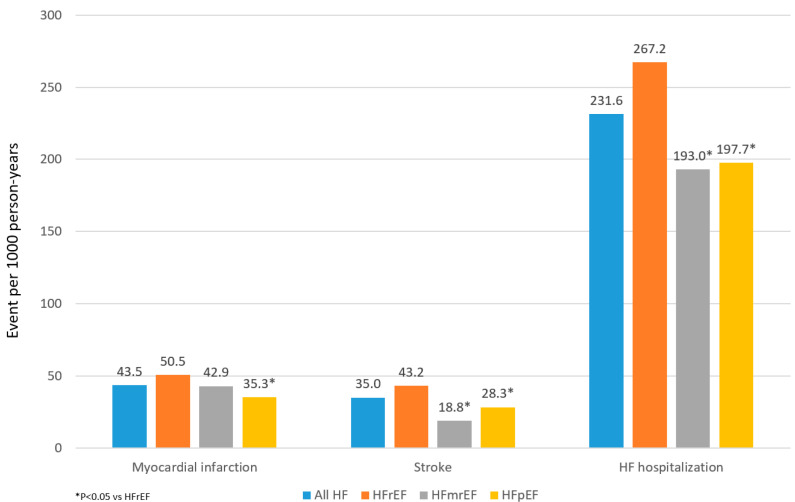
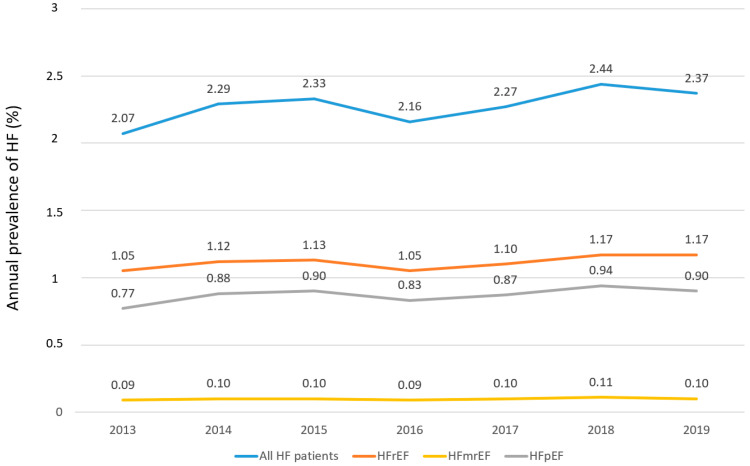
Objective: To estimate the prevalence, incidence, and describe the characteristics and management of patients with heart failure with preserved (HFpEF), mildly reduced (HFmrEF), and reduced ejection fraction (HFrEF) in Spain. Methods: Adults with ≥1 inpatient or outpatient HF diagnosis between 1 January 2013 and 30 September 2019 were identified through the BIG-PAC database. Annual incidence and prevalence by EF phenotype were estimated. Characteristics by EF phenotype were described in the 2016 and 2019 HF prevalent cohorts and outcomes in the 2016 HF prevalent cohort. Results: Overall, HF incidence and prevalence were 0.32/100 person-years and 2.34%, respectively, but increased every year. In 2019, 49.3% had HFrEF, 38.1% had HFpEF, and 4.3% had HFmrEF (in 8.3%, EF was not available). Compared with HFrEF, patients with HFpEF were largely female, older, and had more atrial fibrillation but less atherosclerotic cardiovascular disease. Among patients with HFrEF, 76.3% were taking renin-angiotensin system inhibitors, 69.5% beta-blockers, 36.8% aldosterone antagonists, 12.5% sacubitril/valsartan and 6.7% SGLT2 inhibitors. Patients with HFpEF and HFmrEF took fewer HF drugs compared to HFrEF. Overall, the event rates of HF hospitalization were 231.6/1000 person-years, which is more common in HFrEF patients. No clinically relevant differences were found in patients with HFpEF, regardless EF (50- < 60% vs. ≥60%). Conclusions: >2% of patients have HF, of which around 50% have HFrEF and 40% have HFpEF. The prevalence of HF is increasing over time. Clinical characteristics by EF phenotype are consistent with previous studies. The risk of outcomes, particularly HF hospitalization, remains high, likely related to insufficient HF treatment.
评估西班牙射血分数保留的心力衰竭(HFpEF)、轻度降低的心力衰竭(HFmrEF)和射血分数降低的心力衰竭(HFrEF)患者的患病率、发病率,并描述其特征及治疗情况。方法:通过BIG - PAC数据库识别出2013年1月1日至2019年9月30日期间至少有1次住院或门诊心力衰竭诊断的成年人。按射血分数表型估算年发病率和患病率。在2016年和2019年的心力衰竭现患队列中描述射血分数表型的特征,并在2016年心力衰竭现患队列中描述结局。结果:总体而言,心力衰竭的发病率和患病率分别为0.32/100人年和2.34%,且逐年上升。2019年,49.3%为HFrEF,38.1%为HFpEF,4.3%为HFmrEF(8.3%的患者射血分数数据缺失)。与HFrEF相比,HFpEF患者大多为女性且年龄较大,心房颤动更多,但动脉粥样硬化性心血管疾病较少。在HFrEF患者中,76.3%服用肾素 - 血管紧张素系统抑制剂,69.5%服用β受体阻滞剂,36.8%服用醛固酮拮抗剂,12.5%服用沙库巴曲/缬沙坦,6.7%服用钠 - 葡萄糖协同转运蛋白2(SGLT2)抑制剂。与HFrEF相比,HFpEF和HFmrEF患者服用的心力衰竭药物较少。总体而言,心力衰竭住院事件发生率为231.6/1000人年,在HFrEF患者中更为常见。无论射血分数如何(50 - <60% 与≥60%),HFpEF患者均未发现临床相关差异。结论:超过2%的患者患有心力衰竭,其中约50%为HFrEF,40%为HFpEF。心力衰竭的患病率随时间增加。射血分数表型的临床特征与既往研究一致。结局风险,尤其是心力衰竭住院风险仍然很高,可能与心力衰竭治疗不足有关。