Department of Hematology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, China.
Blood Diseases Institute, Xuzhou Medical University, Xuzhou, China.
Front Immunol. 2022 Aug 23;13:943004. doi: 10.3389/fimmu.2022.943004. eCollection 2022.
Glucocorticoids (GCs) are often used to treat cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). The effects of GCs on the efficacy of CAR-T cell treatment in relapsed/refractory multiple myeloma (RRMM) have not been fully established. We evaluated the impact of GCs on clinical outcomes of RRMM patients treated with CAR-T cells.
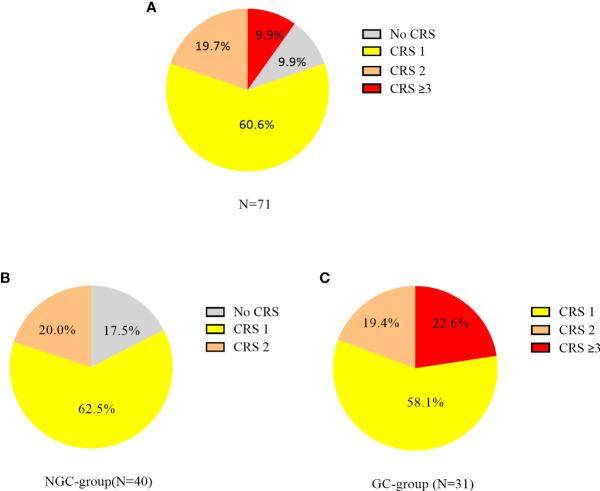
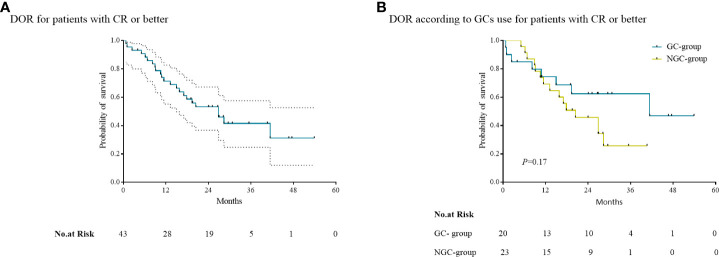
This study involved RRMM patients treated with CAR-T cells at our center between June 2017 and December 2020. Patients were stratified into GC-used group (GC-group) and non-GC-used group (NGC-group). CRS or ICANS was graded on the basis of the American Society of Transplantation and Cellular Therapy consensus grading system. Response status was evaluated by the IMWG Uniform Response Criteria. The duration of response (DOR), progression-free survival (PFS), and overall survival (OS) were calculated.
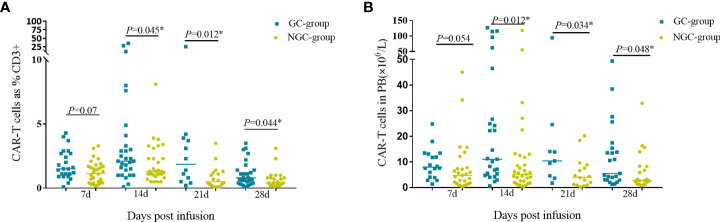
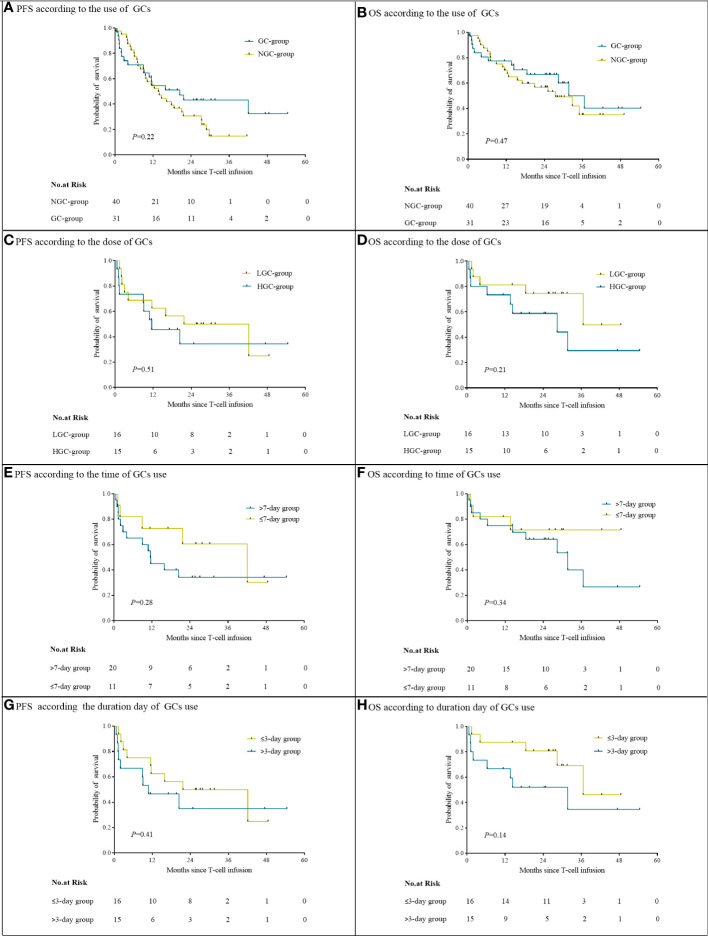
A total of 71 patients were included in this study. In the NGC group (40 patients), 34 (85%) had responses to CAR-T cell therapy, including 16 (40%) stringent complete response (sCR), seven (17.5%) complete response (CR), five (12.5%) very good partial response (VGPR), and six (15%) partial response (PR). The overall response rate (ORR) and complete response rate (CRR) in the NGC group were 85% and 57.5%. In the GC group (31 patients), 29 (93.5%) had responses, including 11 (35.5%) sCR, nine (29%) CR, two (6.4%) VGPR, and seven (22.6%) PR. Differences in ORR and CRR between the two groups were insignificant. The dose, duration, and timing of GCs did not affect ORR and CRR. At a median follow-up of 28.2 months, the median PFS was 20.4 months (95% CI, 7.9 to 32.9) while the median OS was 36.6 months (95% CI, 25.9 to 47.2) for the GC group. The median PFS and OS for the NGC group were 13.7 months (95% CI, 8.8 to 18.6) and 27.5 months (95% CI, 14.1 to 41.0). There were no significant differences in either PFS or OS between the GC group and the NGC group. Differences in median DOR for the patients with CR or better in the GC group and NGC group were not significant ( = 0.17). Earlier, prolonged use and high dose of GCs were not associated with any effects on either PFS or OS. Additionally, GCs had no effects on CAR-T cell proliferation.
Administration of GCs, dose, timing, and duration does not influence the clinical efficacy of CAR-T cells in RRMM in this study.
糖皮质激素(GCs)常用于治疗细胞因子释放综合征(CRS)和免疫效应细胞相关神经毒性综合征(ICANS)。GCs 对复发/难治性多发性骨髓瘤(RRMM)患者 CAR-T 细胞治疗疗效的影响尚未完全确定。我们评估了 GCs 对接受 CAR-T 细胞治疗的 RRMM 患者临床结局的影响。
本研究纳入了 2017 年 6 月至 2020 年 12 月在我中心接受 CAR-T 细胞治疗的 RRMM 患者。患者分为 GC 使用组(GC 组)和非 GC 使用组(NGC 组)。根据美国移植和细胞治疗协会共识分级系统对 CRS 或 ICANS 进行分级。根据国际骨髓瘤工作组统一缓解标准评估缓解状态。计算缓解持续时间(DOR)、无进展生存期(PFS)和总生存期(OS)。
本研究共纳入 71 例患者。在 NGC 组(40 例)中,34 例(85%)对 CAR-T 细胞治疗有反应,包括 16 例(40%)严格完全缓解(sCR)、7 例(17.5%)完全缓解(CR)、5 例(12.5%)非常好的部分缓解(VGPR)和 6 例(15%)部分缓解(PR)。NGC 组的总缓解率(ORR)和完全缓解率(CRR)分别为 85%和 57.5%。在 GC 组(31 例)中,29 例(93.5%)有反应,包括 11 例(35.5%)sCR、9 例(29%)CR、2 例(6.4%)VGPR 和 7 例(22.6%)PR。两组之间 ORR 和 CRR 差异无统计学意义。GC 的剂量、持续时间和时机均未影响 ORR 和 CRR。中位随访 28.2 个月时,GC 组的中位 PFS 为 20.4 个月(95%CI,7.9 至 32.9),中位 OS 为 36.6 个月(95%CI,25.9 至 47.2)。NGC 组的中位 PFS 和 OS 分别为 13.7 个月(95%CI,8.8 至 18.6)和 27.5 个月(95%CI,14.1 至 41.0)。GC 组和 NGC 组之间的 PFS 或 OS 无显著差异。GC 组和 NGC 组中 CR 或更好缓解患者的中位 DOR 差异无统计学意义( = 0.17)。早期、延长使用和高剂量 GC 与 PFS 或 OS 均无相关性。此外,GC 对 CAR-T 细胞增殖无影响。
在本研究中,GC 的使用、剂量、时机和持续时间并不影响 RRMM 患者 CAR-T 细胞的临床疗效。