Loberger Jeremy M, Campbell Caitlin M, Colleti José, Borasino Santiago, Abu-Sultaneh Samer, Khemani Robinder G
Department of Pediatrics, Division of Pediatric Critical Care Medicine University of Alabama at Birmingham, Birmingham, AL.
University of Alabama at Birmingham School of Nursing, Birmingham, AL.
Crit Care Explor. 2022 Sep 2;4(9):e0756. doi: 10.1097/CCE.0000000000000756. eCollection 2022 Sep.
Pediatric ventilation liberation has limited evidence, likely resulting in wide practice variation. To inform future work, practice patterns must first be described.
Describe international pediatric ventilation liberation practices and regional practice variation.
International cross-sectional electronic survey. Nontrainee pediatric medical and cardiac critical care physicians.
Practices focusing on spontaneous breathing trial (SBT) eligibility, SBT practice, non-SBT extubation readiness bundle elements, and post-extubation respiratory support.
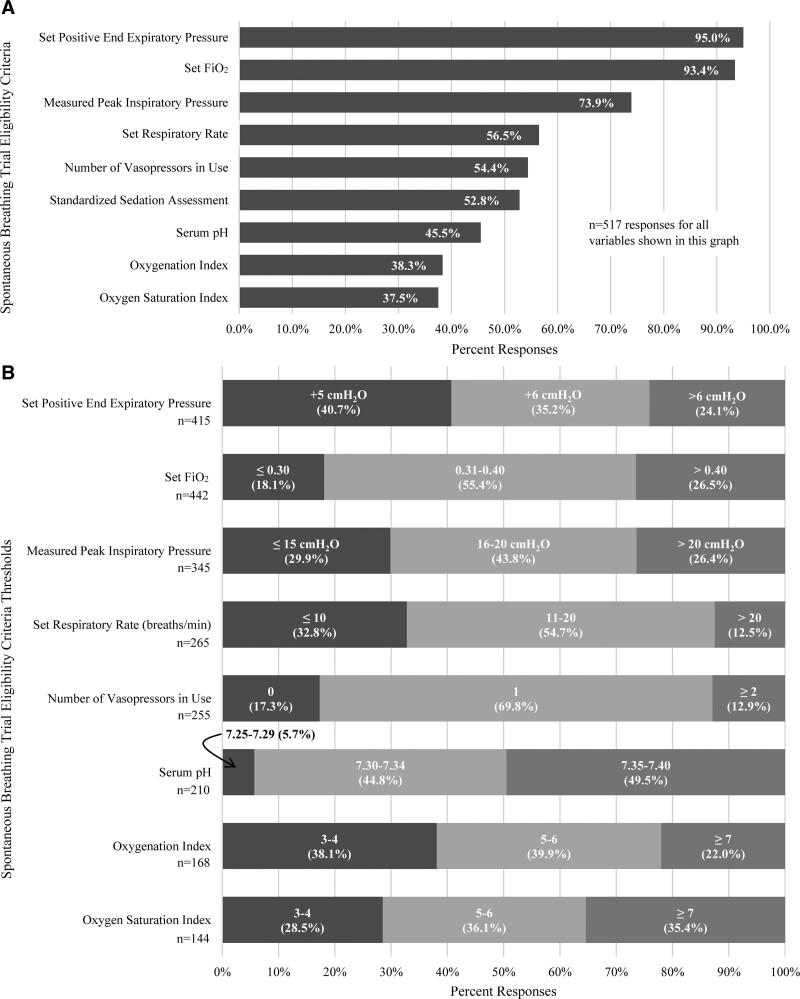
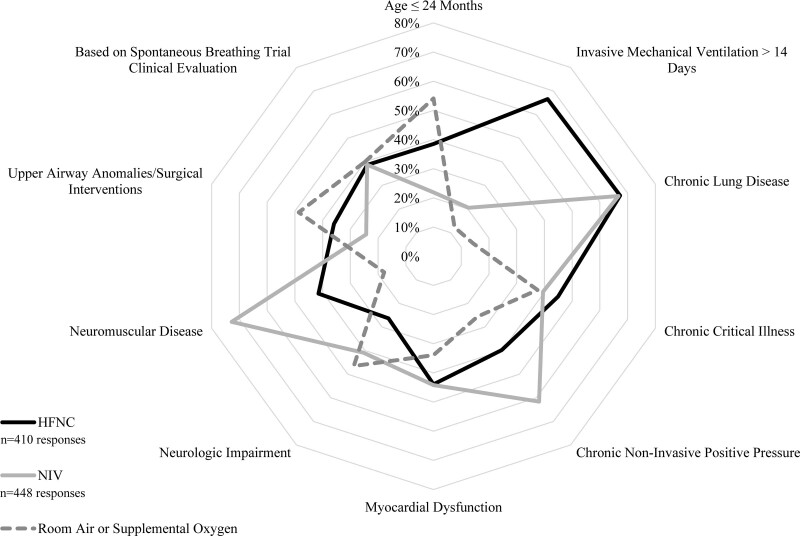
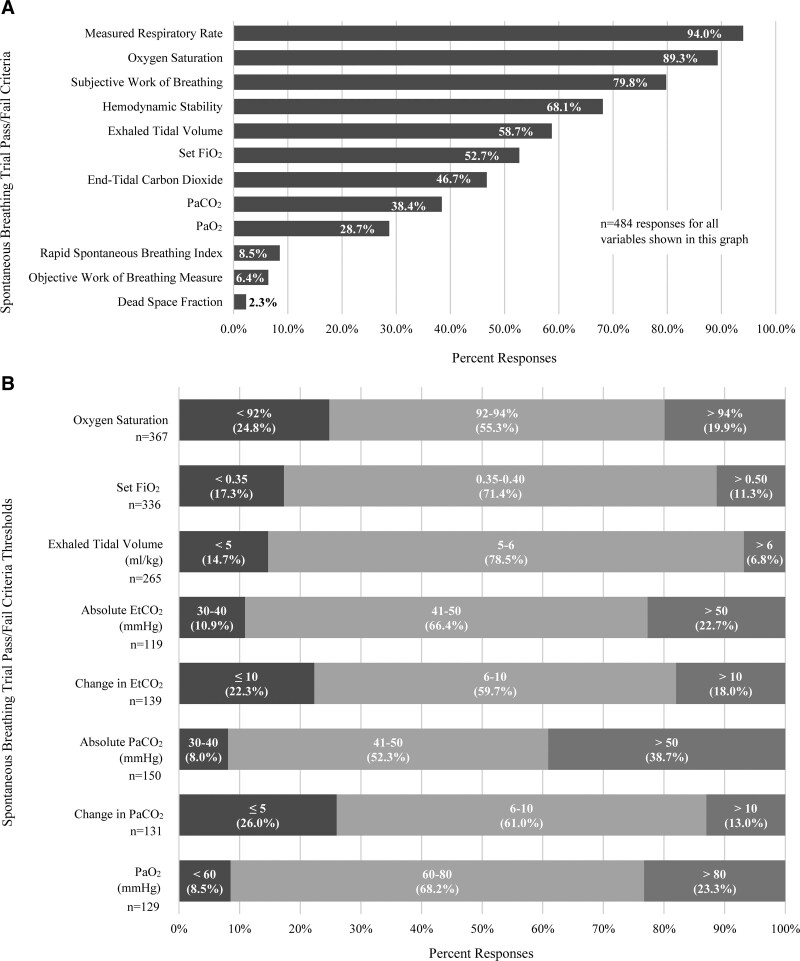
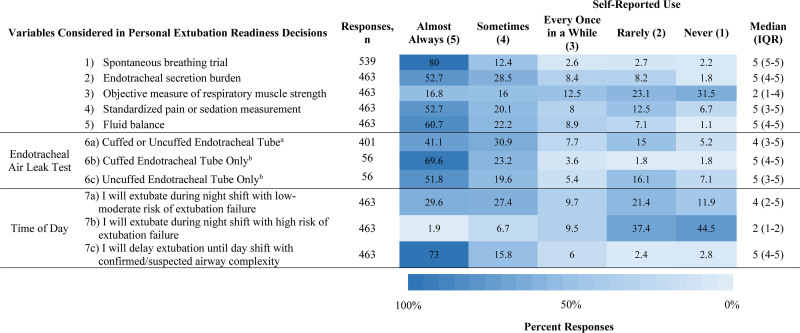
Five-hundred fifty-five responses representing 47 countries were analyzed. Most respondents reported weaning followed by an SBT (86.4%). The top SBT eligibility variables reported were positive end-expiratory pressure (95%), Fio (93.4%), and peak inspiratory pressure (73.9%). Most reported use of standardized pressure support regardless of endotracheal tube size (40.4%) with +10 cm HO predominating (38.6%). SBT durations included less than or equal to 30 minutes (34.8%), 31 minutes to 1 hour (39.3%), and greater than 1 hours (26%). In assigning an SBT result, top variables were respiratory rate (94%), oxygen saturation (89.3%), and subjective work of breathing (79.8%). Most reported frequent consideration of endotracheal secretion burden (81.3%), standardized pain/sedation measurement (72.8%), fluid balance (83%), and the endotracheal air leak test as a part of extubation readiness bundles. Most reported using planned high flow nasal cannula in less than or equal to 50% of extubations (83.2%). Top subpopulations supported with planned HFNC were those with chronic lung disease (67.3%), exposed to invasive ventilation greater than 14 days (66.6%), and chronic critical illness (44.9%). Most reported using planned noninvasive ventilation (NIV) following less than or equal to 20% of extubations (79.9%). Top subpopulations supported with planned NIV were those with neuromuscular disease (72.8%), chronic lung disease (66.7%), and chronic NIV use for any reason (61.6%). Regional variation was high for most practices studied.
International pediatric ventilation liberation practices are heterogeneous. Future study is needed to address key evidence gaps. Many practice differences were associated with respondent region, which must be considered in international study design.
儿科通气撤机的证据有限,这可能导致广泛的实践差异。为指导未来的工作,必须首先描述实践模式。
描述国际儿科通气撤机实践及区域实践差异。
设计、背景与参与者:国际横断面电子调查。非实习儿科医学和心脏重症监护医师。
关注自主呼吸试验(SBT)的适宜性、SBT实践、非SBT拔管准备综合要素以及拔管后呼吸支持的实践。
分析了代表47个国家的555份回复。大多数受访者报告称先进行撤机再进行SBT(86.4%)。报告的SBT适宜性的首要变量为呼气末正压(95%)、吸入氧浓度(93.4%)和吸气峰压(73.9%)。大多数人报告无论气管插管尺寸如何均使用标准化压力支持(40.4%),以+10cmH₂O为主(38.6%)。SBT持续时间包括小于或等于30分钟(34.8%)、31分钟至1小时(39.3%)以及大于1小时(26%)。在判定SBT结果时,首要变量为呼吸频率(94%)、氧饱和度(89.3%)和主观呼吸功(79.8%)。大多数人报告在拔管准备综合要素中经常考虑气管内分泌物负担(81.3%)、标准化疼痛/镇静测量(72.8%)、液体平衡(83%)以及气管漏气试验。大多数人报告在不到或等于50%的拔管中使用计划性高流量鼻导管吸氧(83.2%)。计划性高流量鼻导管吸氧支持的主要亚组为患有慢性肺病的患者(67.3%)、接受有创通气超过14天的患者(66.6%)以及慢性危重病患者(44.9%)。大多数人报告在不到或等于20%的拔管后使用计划性无创通气(NIV)(79.9%)。计划性NIV支持的主要亚组为患有神经肌肉疾病的患者(72.8%)、慢性肺病患者(66.7%)以及因任何原因长期使用NIV的患者(61.6%)。所研究的大多数实践存在较高的区域差异。
国际儿科通气撤机实践存在异质性。需要开展进一步研究以填补关键证据空白。许多实践差异与受访者所在地区有关,在国际研究设计中必须予以考虑。