Faculty of Industrial Engineering and Management, Technion-Israel Institute of Technology, Haifa, Israel.
Faculty of Industrial Engineering and Management, Technion-Israel Institute of Technology, Haifa, Israel.
Lancet Infect Dis. 2023 Jan;23(1):67-73. doi: 10.1016/S1473-3099(22)00527-8. Epub 2022 Sep 9.
The BNT162b2 (Pfizer-BioNTech) two-dose vaccine regiment for children and the BNT162b2 third dose for adolescents were approved shortly before the SARS-CoV-2 omicron (B.1.1.529) outbreak in Israel. We aimed to estimate the effects of these vaccines on the rates of confirmed infection against the omicron variant in children and adolescents.
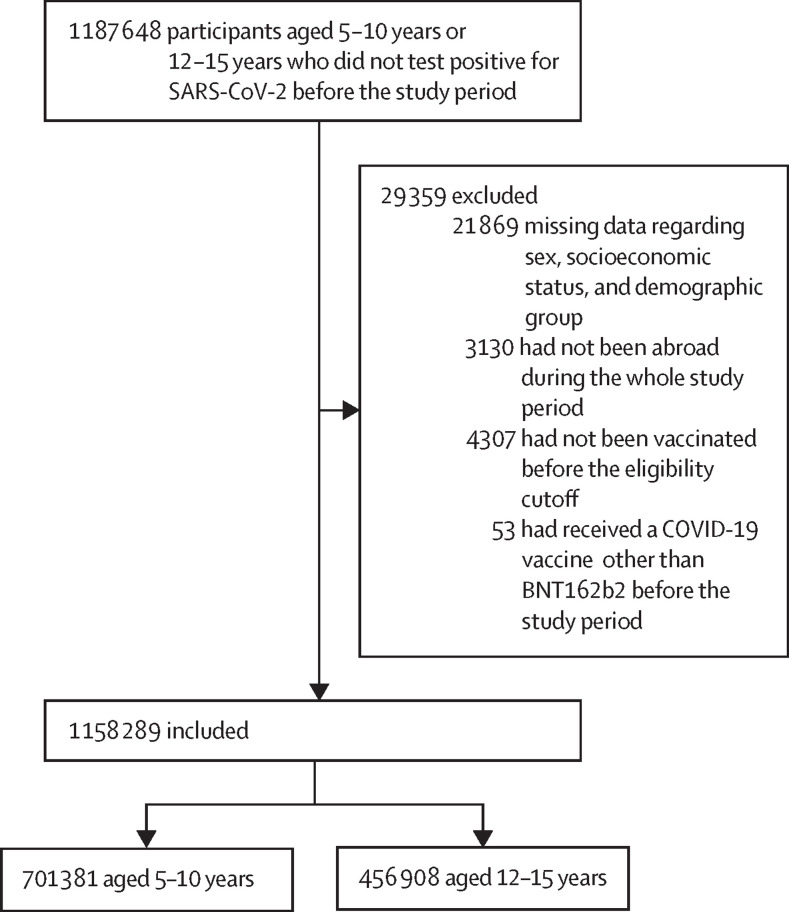
In this observational cohort study, we extracted data for the omicron-dominated (sublineage BA.1) period. We compared rates of confirmed SARS-CoV-2 infection between children aged 5-10 years 14-35 days after receiving the second vaccine dose with an internal control group of children 3-7 days after receiving the first dose (when the vaccine is not yet effective). Similarly, we compared confirmed infection rates in adolescents aged 12-15 years 14-60 days after receiving a booster dose with an internal control group of adolescents 3-7 days after receiving the booster dose. We used Poisson regression, adjusting for age, sex, socioeconomic status, calendar week, and exposure.
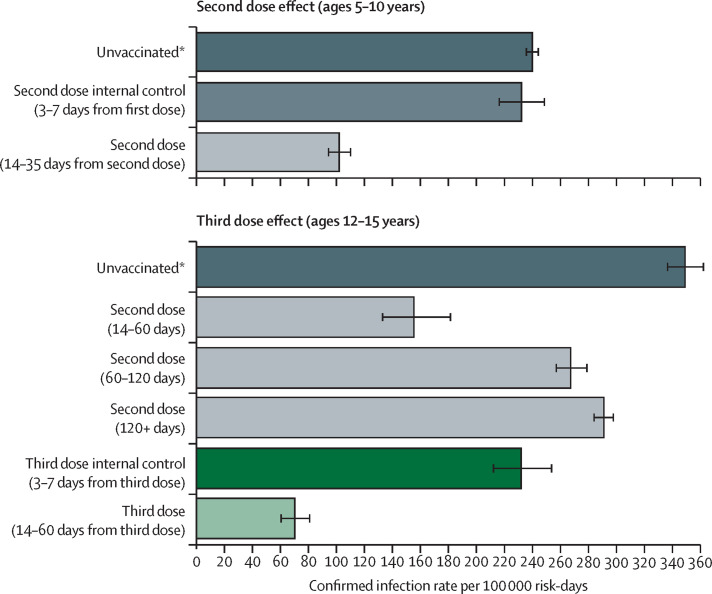
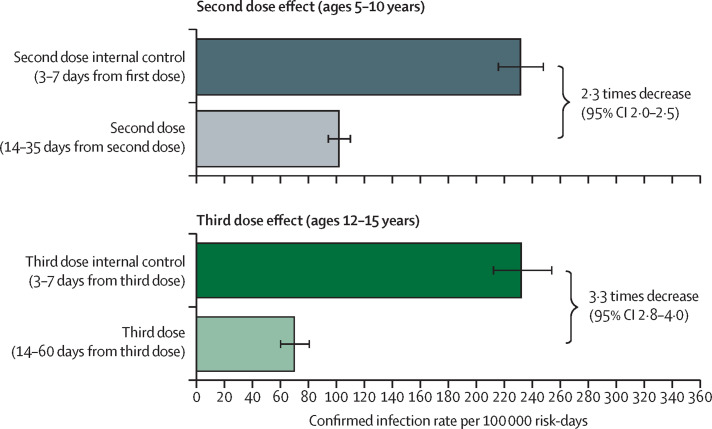
Between Dec 26, 2021, and Jan 8, 2022, we included 1 158 289 participants. In children aged 5-10 years, the adjusted rate of confirmed infection was 2·3 times (95% CI 2·0-2·5) lower in children who received a second dose than in the internal control group. The adjusted infection rate in children who received a second dose was 102 infections per 100 000 risk-days (94-110) compared with 231 infections per 100 000 risk-days (215-248) in the corresponding internal control cohort. In adolescents aged 12-15 years, the booster dose decreased confirmed infection rates by 3·3 times (2·8-4·0) compared with in the internal control group. The adjusted infection rate of the booster cohort was 70 per 100 000 risk-days (60-81) compared with 232 per 100 000 risk-days (212-254) in the internal control cohort.
A recent two-dose vaccination regimen with BNT162b2 and a recent booster dose in adolescents substantially reduced the rate of confirmed infection compared with the internal control groups. Future studies are needed to assess the duration of this protection and protection against other outcomes such as paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 and long-COVID.
None.
在以色列出现 SARS-CoV-2 奥密克戎(B.1.1.529)变体之前不久,批准了用于儿童的 BNT162b2(辉瑞-生物科技)两剂疫苗方案和青少年的 BNT162b2 第三剂疫苗方案。我们旨在评估这些疫苗对儿童和青少年中针对奥密克戎变异体的确诊感染率的影响。
在这项观察性队列研究中,我们提取了奥密克戎占主导地位(亚谱系 BA.1)时期的数据。我们将接受第二剂疫苗后 14-35 天的 5-10 岁儿童与接受第一剂疫苗后 3-7 天的内部对照组(此时疫苗尚未生效)的确诊 SARS-CoV-2 感染率进行比较。同样,我们将接受加强剂量后 14-60 天的 12-15 岁青少年的确诊感染率与接受加强剂量后 3-7 天的内部对照组进行比较。我们使用泊松回归,调整了年龄、性别、社会经济状况、日历周和暴露因素。
在 2021 年 12 月 26 日至 2022 年 1 月 8 日期间,我们纳入了 1158289 名参与者。在 5-10 岁儿童中,与内部对照组相比,接受第二剂疫苗的儿童的确诊感染率低 2.3 倍(95%CI 2.0-2.5)。接受第二剂疫苗的儿童的感染率为每 100000 风险日 102 例(94-110),而相应的内部对照组为每 100000 风险日 231 例(215-248)。在 12-15 岁的青少年中,加强剂量使确诊感染率降低了 3.3 倍(2.8-4.0),与内部对照组相比。加强剂量组的感染率为每 100000 风险日 70 例(60-81),而内部对照组为每 100000 风险日 232 例(212-254)。
最近的 BNT162b2 两剂疫苗方案和青少年最近的加强剂量方案与内部对照组相比,大大降低了确诊感染率。需要进一步研究来评估这种保护作用的持续时间,以及对其他结果的保护作用,如与 SARS-CoV-2 相关的儿童炎症多系统综合征和长期 COVID。
无。