Taboe Hemaho B, Asare-Baah Michael, Yesmin Afsana, Ngonghala Calistus N
Department of Mathematics, University of Florida, Gainesville, FL, 32611, USA.
Laboratoire de Biomathématiques et d'Estimations Forestières, University of Abomey-Calavi, Cotonou, Benin.
Infect Dis Model. 2022 Dec;7(4):709-727. doi: 10.1016/j.idm.2022.08.006. Epub 2022 Sep 8.
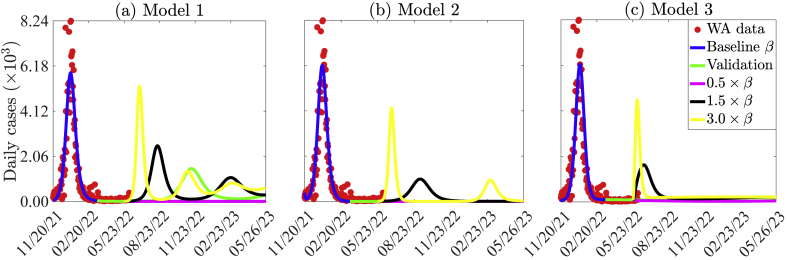
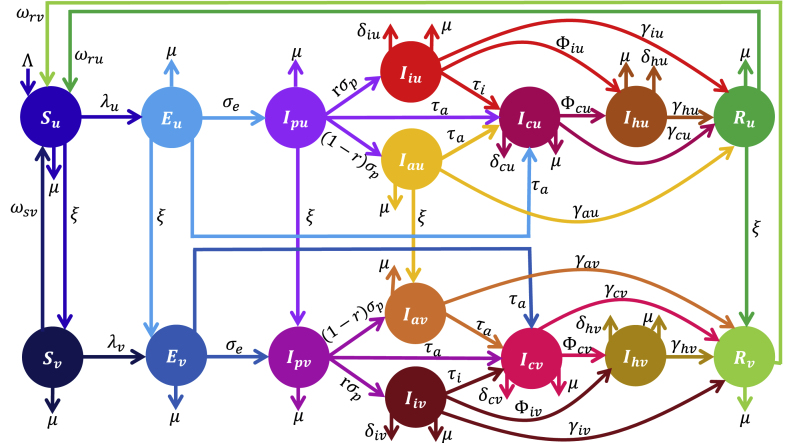
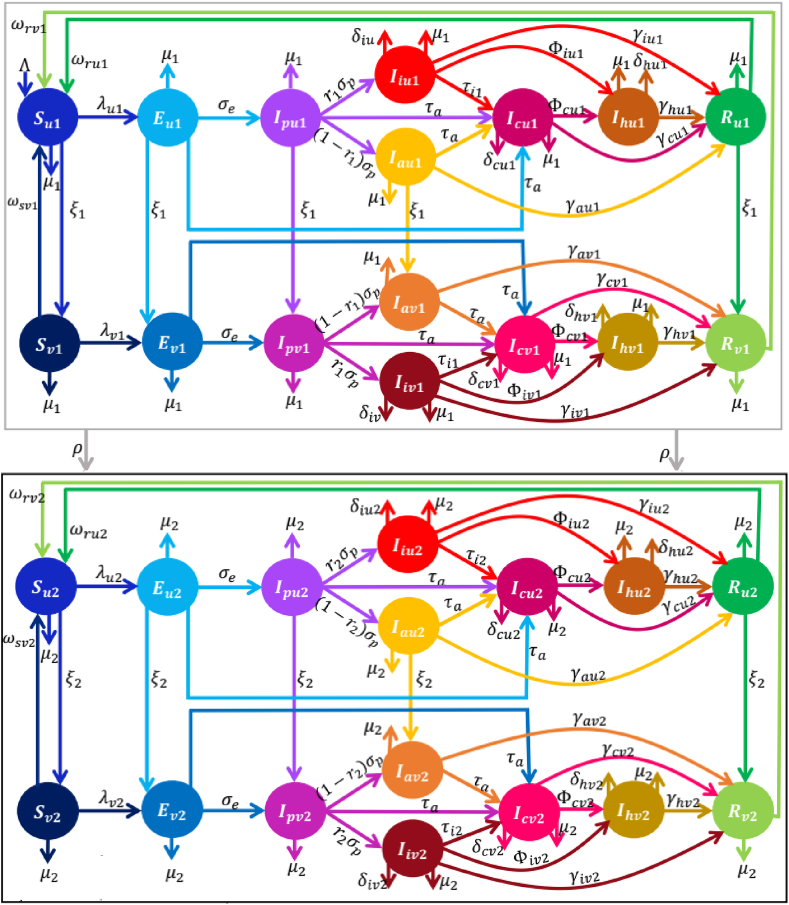
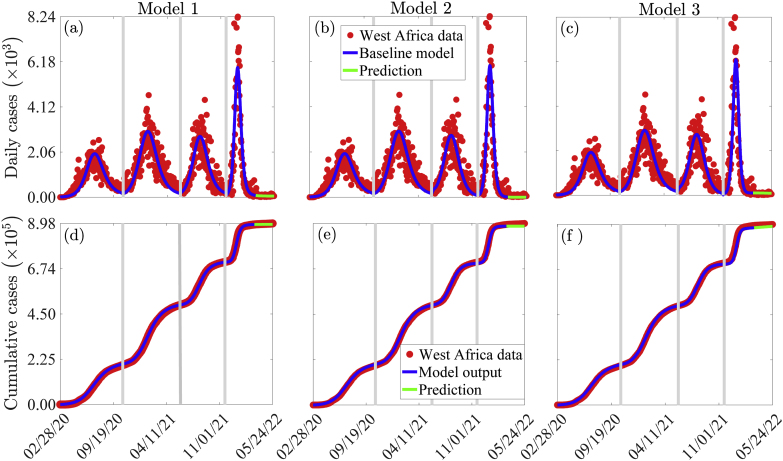
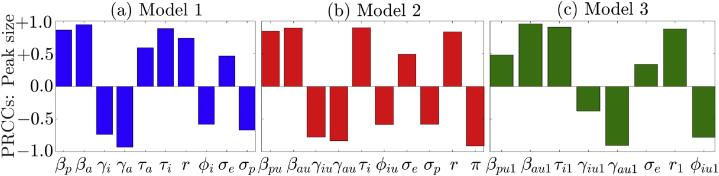
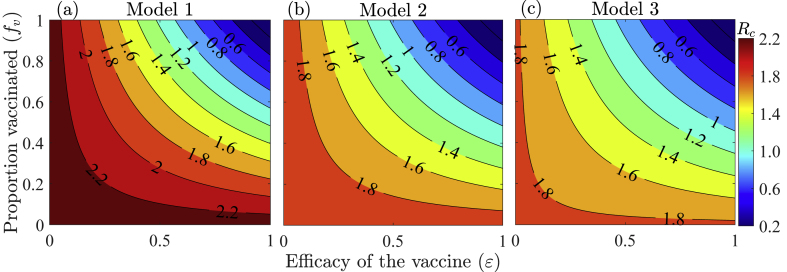
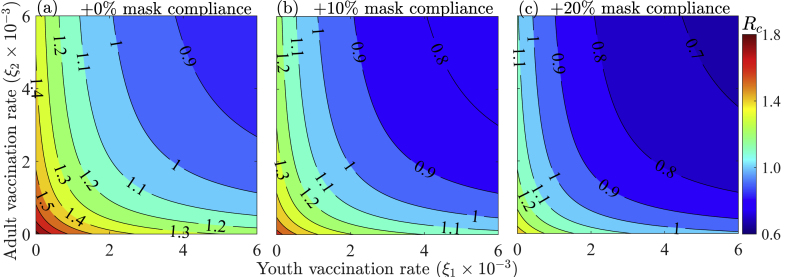
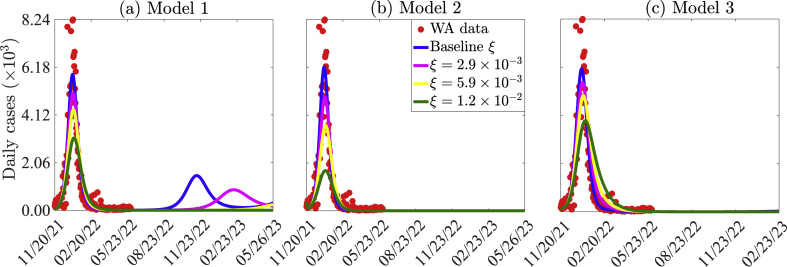
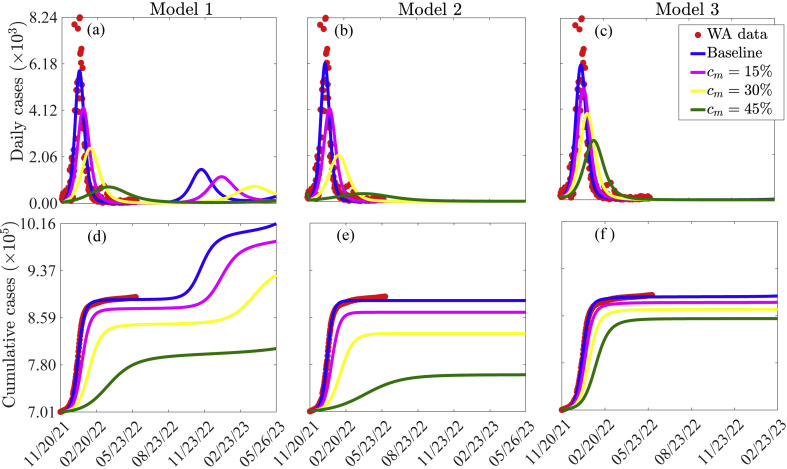
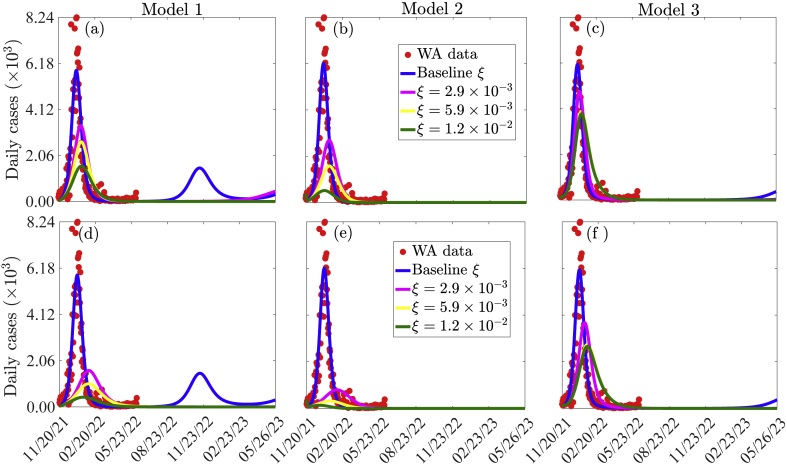
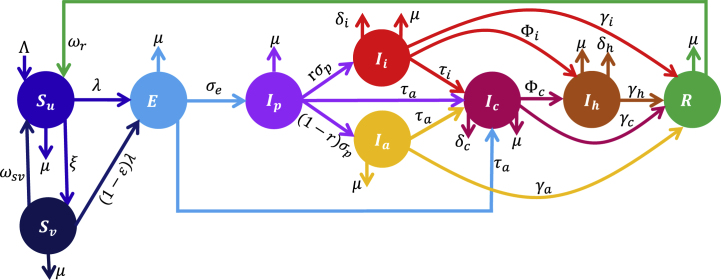
The ongoing COVID-19 pandemic has been a major global health challenge since its emergence in 2019. Contrary to early predictions that sub-Saharan Africa (SSA) would bear a disproportionate share of the burden of COVID-19 due to the region's vulnerability to other infectious diseases, weak healthcare systems, and socioeconomic conditions, the pandemic's effects in SSA have been very mild in comparison to other regions. Interestingly, the number of cases, hospitalizations, and disease-induced deaths in SSA remain low, despite the loose implementation of non-pharmaceutical interventions (NPIs) and the low availability and administration of vaccines. Possible explanations for this low burden include epidemiological disparities, under-reporting (due to limited testing), climatic factors, population structure, and government policy initiatives. In this study, we formulate a model framework consisting of a basic model (in which only susceptible individuals are vaccinated), a vaccine-structured model, and a hybrid vaccine-age-structured model to assess the dynamics of COVID-19 in West Africa (WA). The framework is trained with a portion of the confirmed daily COVID-19 case data for 16 West African countries, validated with the remaining portion of the data, and used to (i) assess the effect of age structure on the incidence of COVID-19 in WA, (ii) evaluate the impact of vaccination and vaccine prioritization based on age brackets on the burden of COVID-19 in the sub-region, and (iii) explore plausible reasons for the low burden of COVID-19 in WA compared to other parts of the world. Calibration of the model parameters and global sensitivity analysis show that asymptomatic youths are the primary drivers of the pandemic in WA. Also, the basic and control reproduction numbers of the hybrid vaccine-age-structured model are smaller than those of the other two models indicating that the disease burden is overestimated in the models which do not account for age-structure. This result is confirmed through the vaccine-derived herd immunity thresholds. In particular, a comprehensive analysis of the basic (vaccine-structured) model reveals that if 84%(73%) of the West African populace is fully immunized with the vaccines authorized for use in WA, vaccine-derived herd immunity can be achieved. This herd immunity threshold is lower (68%) for the hybrid model. Also, all three thresholds are lower (60% for the basic model, 51% for the vaccine-structured model, and 48% for the hybrid model) if vaccines of higher efficacies (e.g., the Pfizer or Moderna vaccine) are prioritized, and higher if vaccines of lower efficacy are prioritized. Simulations of the models show that controlling the COVID-19 pandemic in WA (by reducing transmission) requires a proactive approach, including prioritizing vaccination of more youths or vaccination of more youths and elderly simultaneously. Moreover, complementing vaccination with a higher level of mask compliance will improve the prospects of containing the pandemic. Additionally, simulations of the model predict another COVID-19 wave (with a smaller peak size compared to the Omicron wave) by mid-July 2022. Furthermore, the emergence of a more transmissible variant or easing the existing measures that are effective in reducing transmission will result in more devastating COVID-19 waves in the future. To conclude, accounting for age-structure is important in understanding why the burden of COVID-19 has been low in WA and sustaining the current vaccination level, complemented with the WHO recommended NPIs is critical in curbing the spread of the disease in WA.
自2019年出现以来,持续的新冠疫情一直是全球主要的健康挑战。与早期预测相反,早期预测认为撒哈拉以南非洲(SSA)由于该地区易受其他传染病影响、医疗系统薄弱以及社会经济状况,将承担不成比例的新冠疫情负担,但与其他地区相比,疫情在SSA的影响非常轻微。有趣的是,尽管非药物干预(NPIs)实施宽松且疫苗供应和接种率低,SSA的病例数、住院人数和疾病导致的死亡人数仍然很低。造成这种低负担的可能原因包括流行病学差异、报告不足(由于检测有限)、气候因素、人口结构和政府政策举措。在本研究中,我们制定了一个模型框架,包括一个基本模型(其中只有易感个体接种疫苗)、一个疫苗结构模型和一个混合疫苗年龄结构模型,以评估西非(WA)的新冠病毒动态。该框架使用16个西非国家的部分每日确诊新冠病例数据进行训练,用其余数据进行验证,并用于(i)评估年龄结构对WA新冠发病率的影响,(ii)评估基于年龄组的疫苗接种和疫苗优先级对该次区域新冠负担的影响,以及(iii)探究WA与世界其他地区相比新冠负担较低的合理原因。模型参数校准和全局敏感性分析表明,无症状青年是WA疫情的主要驱动因素。此外,混合疫苗年龄结构模型的基本再生数和控制再生数小于其他两个模型,这表明在不考虑年龄结构的模型中疾病负担被高估了。这一结果通过疫苗衍生的群体免疫阈值得到证实。特别是,对基本(疫苗结构)模型的综合分析表明,如果84%(73%)的西非民众用在WA获批使用的疫苗完全免疫,就可以实现疫苗衍生的群体免疫。混合模型的这一群体免疫阈值较低(68%)。此外,如果优先使用更高效力的疫苗(例如辉瑞或莫德纳疫苗),所有三个阈值都较低(基本模型为60%,疫苗结构模型为51%,混合模型为48%),如果优先使用效力较低的疫苗,则阈值较高。模型模拟表明,在WA控制新冠疫情(通过减少传播)需要积极主动的方法,包括优先为更多青年接种疫苗或同时为更多青年和老年人接种疫苗。此外,通过更高水平的口罩佩戴依从性来补充疫苗接种将改善控制疫情的前景。此外,模型模拟预测到2022年7月中旬将出现另一波新冠疫情(与奥密克戎波相比峰值规模较小)。此外,出现更具传播性的变体或放松现有的有效减少传播的措施将导致未来更具毁灭性的新冠疫情浪潮。总之,考虑年龄结构对于理解为什么WA的新冠负担一直较低很重要,维持当前的疫苗接种水平,并辅以世界卫生组织推荐的非药物干预措施对于遏制WA的疾病传播至关重要。