University Medical Center Rotterdam, Erasmus MC, Department of Public Health, Rotterdam, the Netherlands.
Department of Pathology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, the Netherlands.
Cancer Epidemiol Biomarkers Prev. 2023 Feb 6;32(2):183-192. doi: 10.1158/1055-9965.EPI-22-0712.
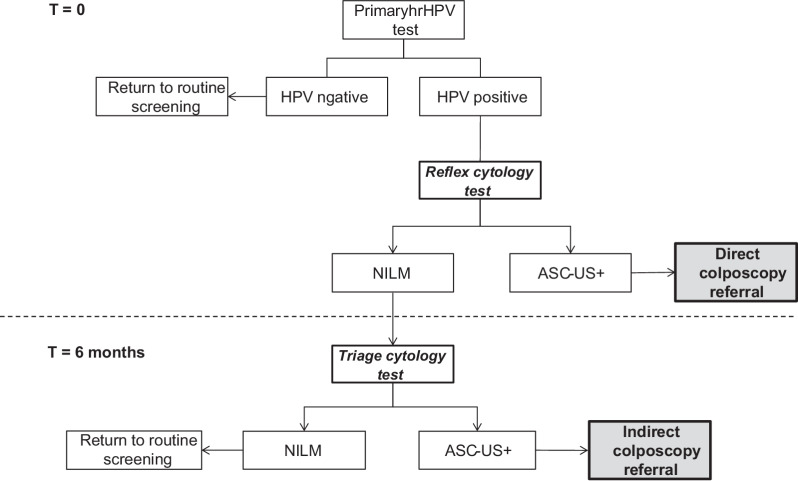
In the Netherlands, lower high-risk human papillomavirus (hrHPV) positivity but higher cervical intraepithelial neoplasia (CIN) 2+ detection were found in self-collected compared with clinician-collected samples. To investigate the possible reason for these differences, we compared sociodemographic and screening characteristics of women and related these to screening outcomes.
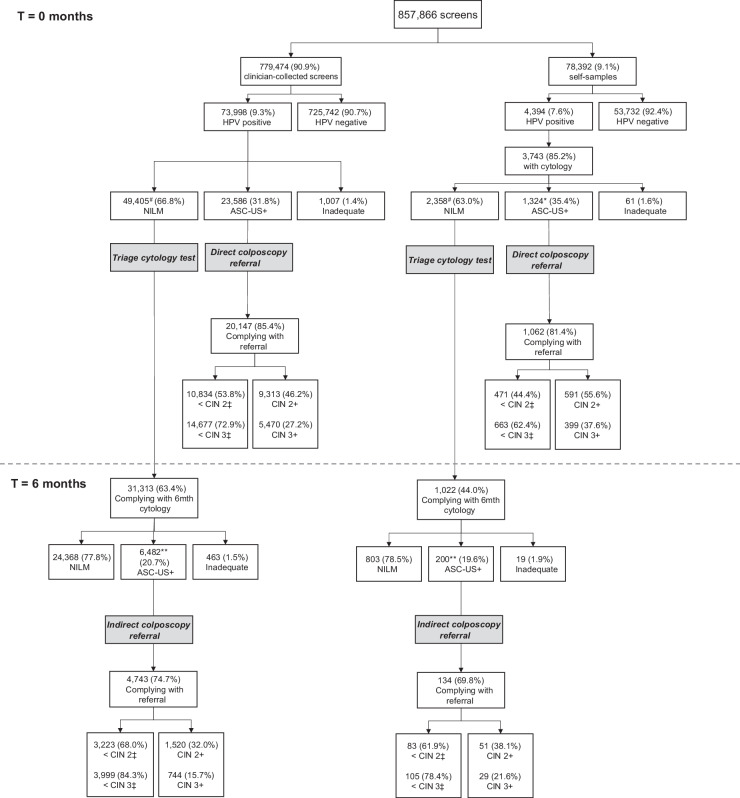
We extracted data from PALGA on all primary hrHPV screens and associated follow-up tests for 857,866 screened women, invited in 2017 and 2018. We linked these data with sociodemographic data from Statistics Netherlands. Logistic regression was performed for hrHPV positivity and CIN 2+/3+ detection.
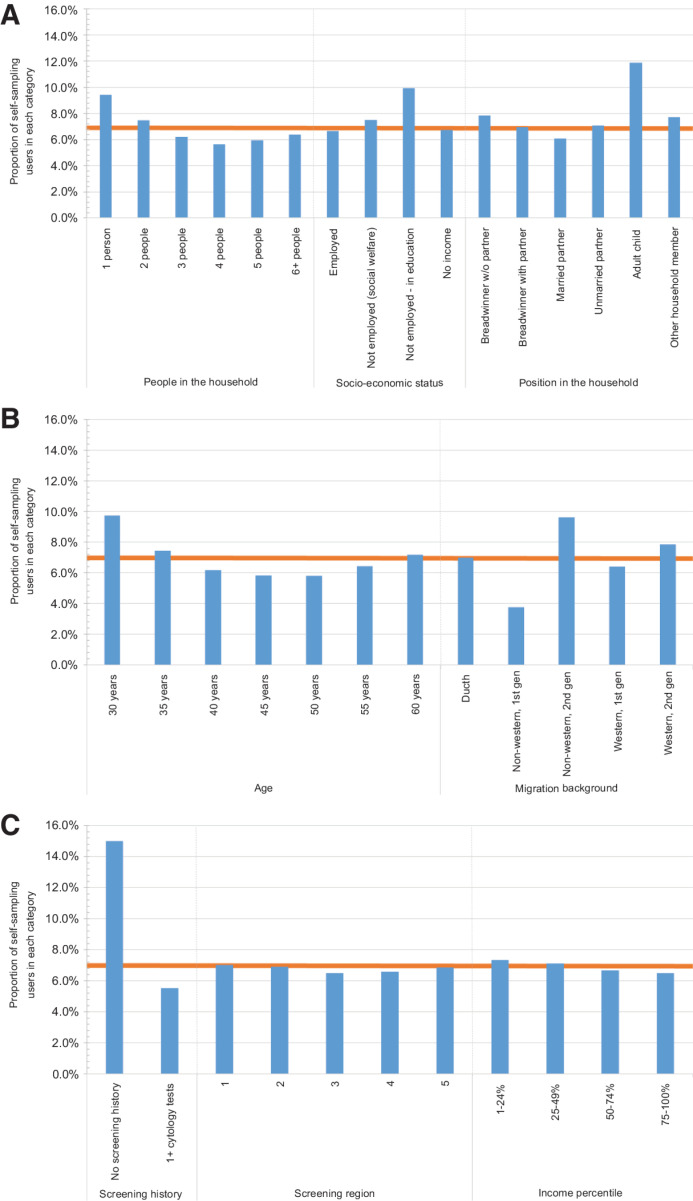
Out of the 857,866 women, 6.8% chose to use a self-sampling device. A higher proportion of self-sampling users was ages 30 to 35 years, was not previously screened, was living in a one-person household, or was the breadwinner in the household. After adjustment for these factors self-sampling had lower hrHPV positivity (aOR, 0.65; 95% CI, 0.63-0.68)) as compared with clinician-collected sampling, as well as lower odds of CIN 2+ (aOR, 0.76; 95% CI, 0.70-0.82) and CIN 3+ (aOR, 0.86; 95% CI, 0.78-0.95) detection.
It is likely that the observed differences between the two sampling methods are not only related to sociodemographic differences, but related to differences in screening test accuracy and/or background risk.
Self-sampling can be used for targeting underscreened women, as a more convenient screening tool. Further investigation is required to evaluate how to implement self-sampling, when it is used as a primary instrument in routine screening. See related commentary by Arbyn et al., p. 159.
在荷兰,与医生采集样本相比,自我采集样本的高危型人乳头瘤病毒(hrHPV)阳性率较低,但宫颈上皮内瘤变(CIN)2+的检出率较高。为了探究这些差异的可能原因,我们比较了女性的社会人口统计学和筛查特征,并将这些特征与筛查结果相关联。
我们从 PALGA 中提取了 2017 年和 2018 年邀请的 857866 名筛查女性的所有初次 hrHPV 筛查和相关随访检测数据。我们将这些数据与荷兰统计局的社会人口统计学数据进行了关联。我们对 hrHPV 阳性和 CIN 2+/3+检测结果进行了逻辑回归分析。
在 857866 名女性中,有 6.8%的人选择使用自我采样设备。与医生采集样本相比,自我采样设备使用者更多的是年龄在 30 至 35 岁之间、从未接受过筛查、独居或家庭收入主要来源的人群。在调整了这些因素后,自我采样的 hrHPV 阳性率(优势比,0.65;95%置信区间,0.63-0.68)以及 CIN 2+(优势比,0.76;95%置信区间,0.70-0.82)和 CIN 3+(优势比,0.86;95%置信区间,0.78-0.95)的检出率均较低。
两种采样方法之间的差异可能不仅与社会人口统计学差异有关,还与筛查试验的准确性和/或背景风险有关。
自我采样可用于针对筛查不足的女性,作为一种更方便的筛查工具。需要进一步研究如何实施自我采样,当它作为常规筛查的主要手段时。见 Arbin 等人的相关评论,第 159 页。