Department of Liver Surgery, West China Hospital, Sichuan University, Chengdu, 610041, Sichuan, China.
Department of General Surgery, The First People's Hospital of Longquanyi District, Chengdu, 610041, Sichuan, China.
BMC Surg. 2022 Sep 13;22(1):339. doi: 10.1186/s12893-022-01789-4.
Liver cirrhosis is a well-known risk factor for carcinogenesis of hepatocellular carcinoma (HCC). The aim of the present study was to construct individual prognostic models for HCC with cirrhosis.
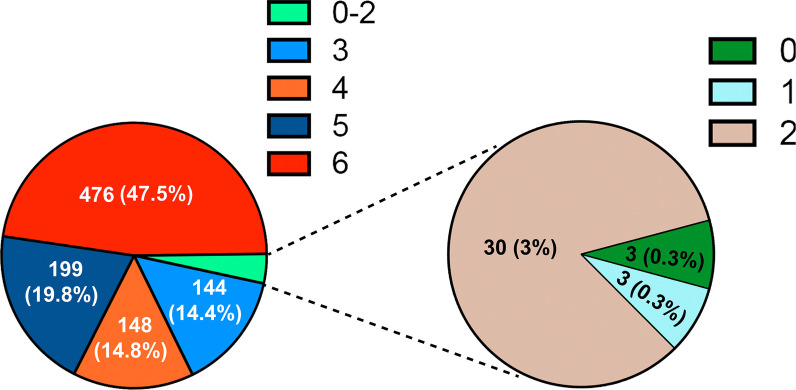
The clinical differences between HCC patients with and without cirrhosis were compared using a large cohort of 1003 cases. The patients with cirrhosis were randomly divided into a training cohort and a validation cohort in a ratio of 2:1. Univariate and multivariate analyses were performed to reveal the independent risk factors for recurrence-free survival (RFS) and overall survival (OS) in HCC patients with cirrhosis. These factors were subsequently used to construct nomograms.
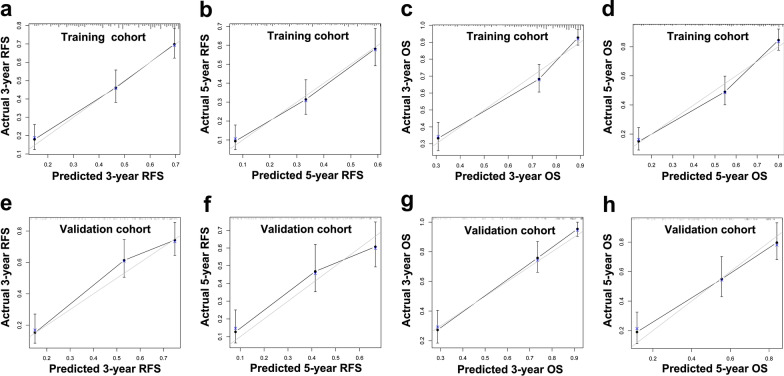
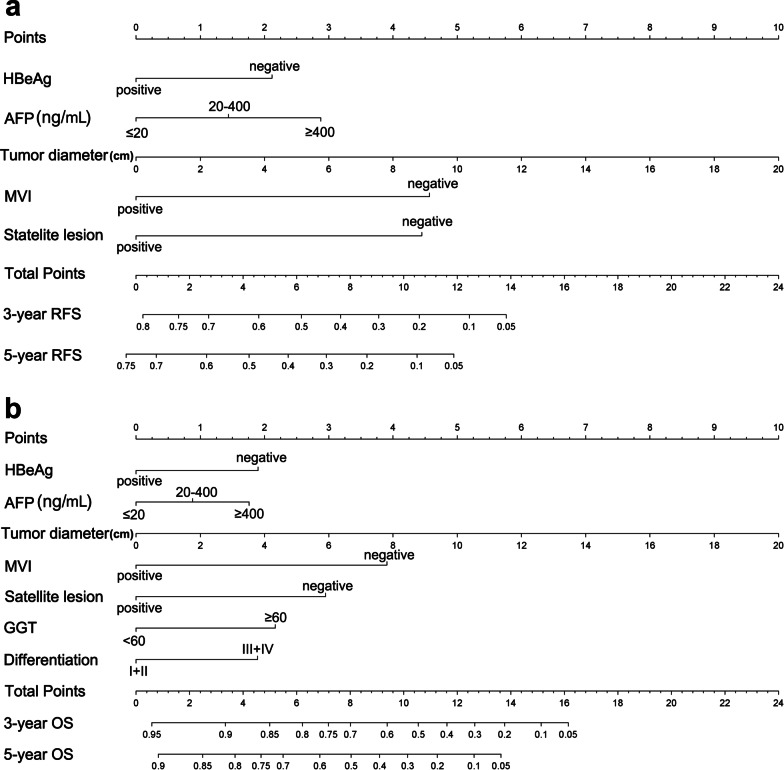
Multivariate analyses revealed that five clinical variables (hepatitis B e antigen (HBeAg) positivity, alpha-fetoprotein (AFP) level, tumour diameter, microvascular invasion (MVI), and satellite lesions) and seven variables (HBeAg positivity, AFP level, tumour diameter, MVI, satellite lesions, gamma-glutamyl transpeptidase level, and histological differentiation) were significantly associated with RFS and OS, respectively. The C-indices of the nomograms for RFS and OS were 0.739 (P < 0.001) and 0.789 (P < 0.001), respectively, in the training cohort, and 0.752 (P < 0.001) and 0.813 (P < 0.001), respectively, in the validation cohort. The C-indices of the nomograms were significantly higher than those of conventional staging systems (P < 0.001). The calibration plots showed optimal consistence between the nomogram-predicted and observed prognoses.
The nomograms developed in the present study showed good performance in predicting the prognoses of HCC patients with hepatitis B virus-associated cirrhosis.
肝硬化是肝细胞癌(HCC)发生癌变的已知危险因素。本研究的目的是为肝硬化合并 HCC 患者构建个体化预后模型。
利用包含 1003 例患者的大型队列比较了 HCC 患者中伴有和不伴有肝硬化的临床差异。肝硬化患者按 2:1 的比例随机分为训练队列和验证队列。进行单因素和多因素分析,以揭示肝硬化合并 HCC 患者无复发生存(RFS)和总生存(OS)的独立预后因素。随后,这些因素被用于构建列线图。
多因素分析显示,5 个临床变量(乙型肝炎 e 抗原(HBeAg)阳性、甲胎蛋白(AFP)水平、肿瘤直径、微血管侵犯(MVI)和卫星病变)和 7 个变量(HBeAg 阳性、AFP 水平、肿瘤直径、MVI、卫星病变、γ-谷氨酰转肽酶水平和组织学分级)分别与 RFS 和 OS 显著相关。训练队列中 RFS 和 OS 列线图的 C 指数分别为 0.739(P<0.001)和 0.789(P<0.001),验证队列中分别为 0.752(P<0.001)和 0.813(P<0.001)。列线图的 C 指数明显高于传统分期系统(P<0.001)。校准图显示列线图预测和观察到的预后之间具有最佳一致性。
本研究中开发的列线图在预测乙型肝炎病毒相关肝硬化合并 HCC 患者的预后方面表现出良好的性能。