University of Chile, Faculty of Medicine, Hospital "Dr. José J. Aguirre", Department of Surgery - Santiago, Chile.
Arq Bras Cir Dig. 2022 Sep 9;35:e1678. doi: 10.1590/0102-672020220002e1678. eCollection 2022.
Laparoscopic Nissen fundoplication fails to control the gastroesophageal reflux in almost 15% of patients, and most of them must be reoperated due to postoperative symptoms. Different surgical options have been suggested.
This study aimed to present the postoperative outcomes of patients submitted to three different procedures: redo laparoscopic Nissen fundoplication alone (Group A), redo laparoscopic Nissen fundoplication combined with distal gastrectomy (Group B), or conversion to laparoscopic Toupet combined with distal gastrectomy with Roux-en-Y gastrojejunostomy (Group C).
This is a prospective study involving 77 patients who were submitted initially to laparoscopic Nissen fundoplication and presented recurrence of gastroesophageal reflux after the operation. They were evaluated before and after the reoperation with clinical questionnaire and objective functional studies. After reestablishing the anatomy of the esophagogastric junction, a surgery was performed. None of the patients were lost during follow-up.
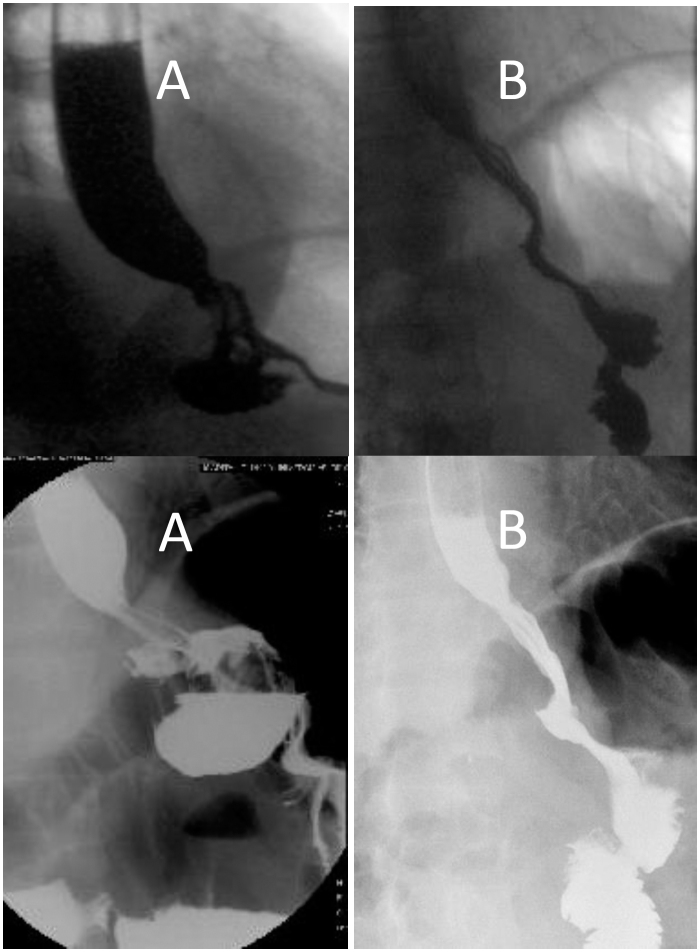
Persistent symptoms were observed more frequently in Group A or B patients, including wrap stricture, intrathoracic wrap, or twisted fundoplication. In Group C, recurrent symptoms associated with this anatomic alteration were infrequently observed. Incompetent lower esophageal sphincter was confirmed in 57.7% of patients included in Group A, compared to 17.2% after Nissen and distal gastrectomy and 26% after Toupet procedure plus distal gastrectomy. In Group C, despite the high percentage of patients with incompetent lower esophageal sphincter, 8.7% had abnormal acid reflux after surgery.
Nissen and Toupet procedures combined with Roux-en-Y distal gastrectomy are safe and effective for the management of failed Nissen fundoplication. However, Toupet technique is preferable for patients suffering from mainly dysphagia and pain.
腹腔镜 Nissen 胃底折叠术未能控制近 15%的胃食管反流患者的症状,其中大多数患者由于术后症状必须再次手术。已经提出了不同的手术选择。
本研究旨在介绍三种不同手术的术后结果:单独再次腹腔镜 Nissen 胃底折叠术(A 组)、再次腹腔镜 Nissen 胃底折叠术联合远端胃切除术(B 组)或转换为腹腔镜 Toupet 联合远端胃切除术加 Roux-en-Y 胃空肠吻合术(C 组)。
这是一项前瞻性研究,涉及 77 例最初接受腹腔镜 Nissen 胃底折叠术但术后出现胃食管反流复发的患者。在再次手术后,通过临床问卷和客观功能研究对他们进行术前和术后评估。在重建食管胃连接部解剖结构后进行手术。在随访期间,没有患者丢失。
A 组或 B 组患者更常出现持续性症状,包括包裹狭窄、胸腔内包裹或扭曲的胃底折叠术。在 C 组中,与这种解剖改变相关的复发性症状很少观察到。在纳入 A 组的 57.7%的患者中确认存在下食管括约肌功能不全,而 Nissen 和远端胃切除术的为 17.2%,Toupet 术加远端胃切除术的为 26%。在 C 组中,尽管下食管括约肌功能不全的患者百分比较高,但仍有 8.7%的患者术后存在异常酸反流。
Nissen 和 Toupet 术联合 Roux-en-Y 远端胃切除术是治疗失败的 Nissen 胃底折叠术的安全有效方法。然而,对于主要有吞咽困难和疼痛的患者,Toupet 技术更可取。