Voleti Navya, Reddy Surya Prakash, Ssentongo Paddy
Department of Medicine, Penn State Health Medical Center, Hershey, PA, United States.
Department of Medicine, Osmania Medical College, Hyderabad, India.
Front Cardiovasc Med. 2022 Aug 29;9:951314. doi: 10.3389/fcvm.2022.951314. eCollection 2022.
This study aimed to compare the incidence of myocarditis in COVID-19 vaccines and in severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) infection groups.
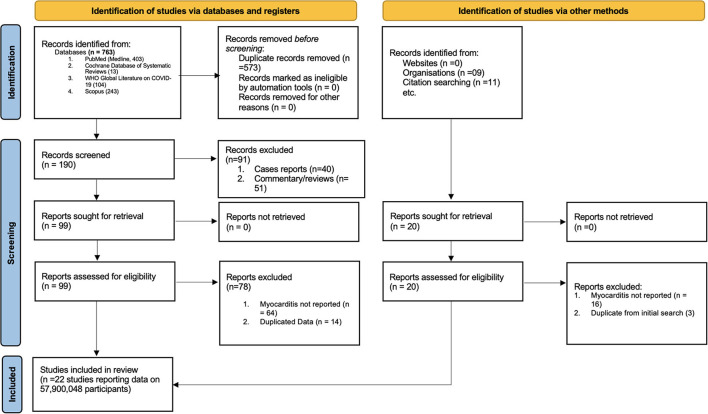
Electronic databases (MEDLINE, Scopus, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and the WHO Global Literature on Coronavirus Disease) and trial registries were searched up to May 2022, for randomized controlled trials and observational cohort studies reporting the risk of myocarditis associated with the COVID-19 vaccines and the risk associated with SARS-CoV-2 infection. We estimated the effect of COVID-19 infection and vaccines on rates of myocarditis by random-effects meta-analyses using the generic inverse variance method. Meta-regression analyses were conducted to assess the effect of sex and age on the incidence of myocarditis.
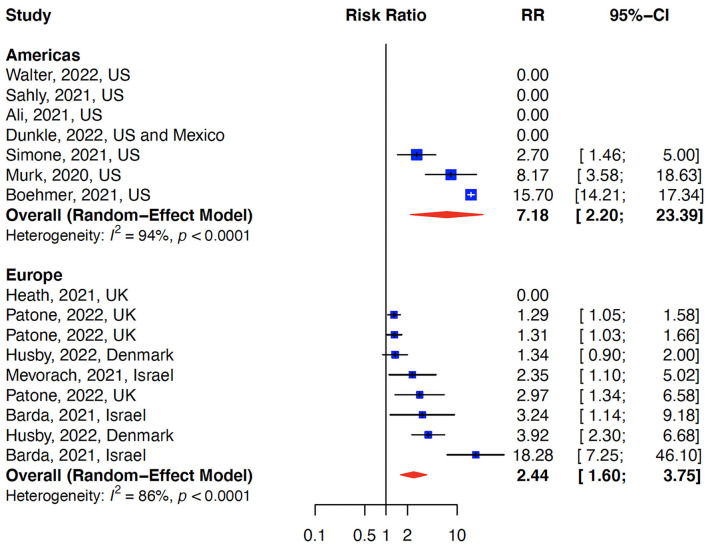
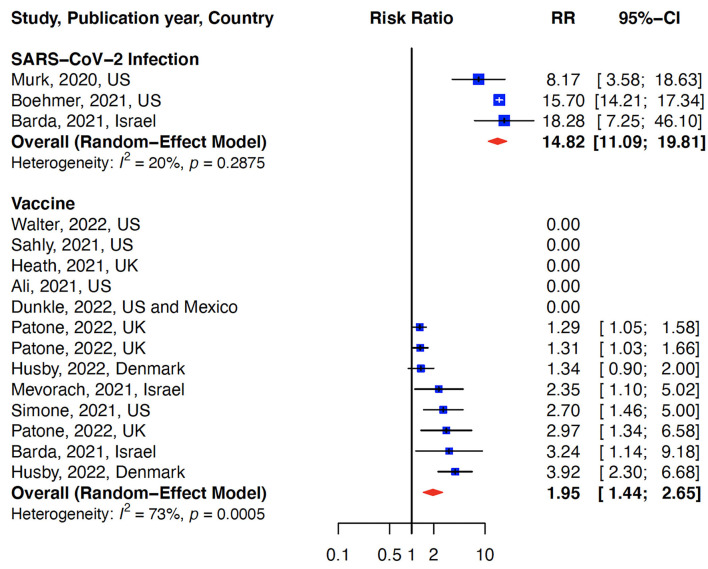
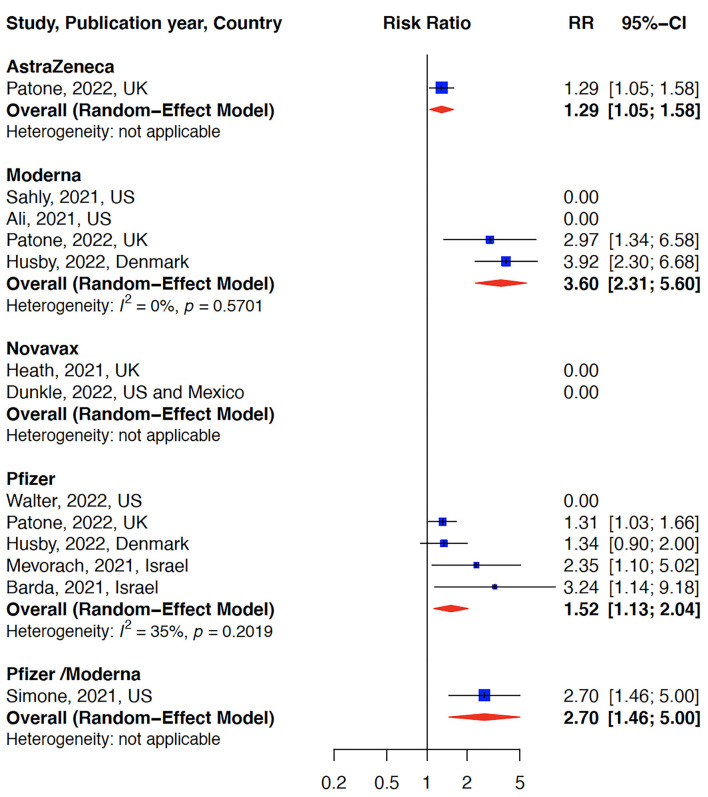
We identified 22 eligible studies consisting of 55.5 million vaccinated cohorts and 2.5 million in the infection cohort. The median age was 49 years (interquartile range (IQR): 38-56), and 49% (IQR: 43 to 52%) were men. Of patients diagnosed with myocarditis (in both vaccination and COVID-19 cohort) 1.07% were hospitalized and 0.015% died. The relative risk (RR) for myocarditis was more than seven times higher in the infection group than in the vaccination group [RR: 15 (95% CI: 11.09-19.81, infection group] and RR: 2 (95% CI: 1.44-2.65, vaccine group). Of patients who developed myocarditis after receiving the vaccine or having the infection, 61% (IQR: 39-87%) were men. Meta-regression analysis indicated that men and younger populations had a higher risk of myocarditis. A slow decline in the rates of myocarditis was observed as a function of time from vaccination. The risk of bias was low.
In this systematic review and meta-analysis, we found that the risk of myocarditis is more than seven fold higher in persons who were infected with the SARS-CoV-2 than in those who received the vaccine. These findings support the continued use of mRNA COVID-19 vaccines among all eligible persons per CDC and WHO recommendations.
本研究旨在比较新型冠状病毒肺炎(COVID-19)疫苗接种组和严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染组中心肌炎的发生率。
检索截至2022年5月的电子数据库(MEDLINE、Scopus、Cochrane对照试验中央注册库、Cochrane系统评价数据库以及世界卫生组织关于冠状病毒病的全球文献)和试验注册库,查找报告与COVID-19疫苗相关的心肌炎风险以及与SARS-CoV-2感染相关风险的随机对照试验和观察性队列研究。我们采用通用逆方差法通过随机效应荟萃分析来估计COVID-19感染和疫苗对心肌炎发生率的影响。进行荟萃回归分析以评估性别和年龄对心肌炎发生率的影响。
我们确定了22项符合条件的研究,其中包括5550万疫苗接种队列和250万感染队列。中位年龄为49岁(四分位间距(IQR):38 - 56岁),49%(IQR:43%至52%)为男性。在被诊断为心肌炎的患者中(疫苗接种组和COVID-19感染组均有),1.07%住院,0.015%死亡。感染组心肌炎的相对风险(RR)比疫苗接种组高出七倍多[RR:15(95%置信区间:11.09 - 19.81,感染组)]和RR:2(95%置信区间:1.44 - 2.65,疫苗组)。在接种疫苗或感染后发生心肌炎的患者中,61%(IQR:39% - 87%)为男性。荟萃回归分析表明男性和较年轻人群患心肌炎的风险更高。观察到心肌炎发生率随接种疫苗后的时间推移呈缓慢下降趋势。偏倚风险较低。
在本系统评价和荟萃分析中,我们发现感染SARS-CoV-2的人群患心肌炎的风险比接种疫苗的人群高出七倍多。这些发现支持按照美国疾病控制与预防中心(CDC)和世界卫生组织(WHO)的建议,在所有符合条件的人群中继续使用mRNA COVID-19疫苗。