Department of Cardiology Radboud University Medical Center Nijmegen The Netherlands.
Department of Cardiology Cardiovascular Research Institute (CARIM), Maastricht University Medical Center Maastricht The Netherlands.
J Am Heart Assoc. 2022 Oct 4;11(19):e025106. doi: 10.1161/JAHA.121.025106. Epub 2022 Sep 21.
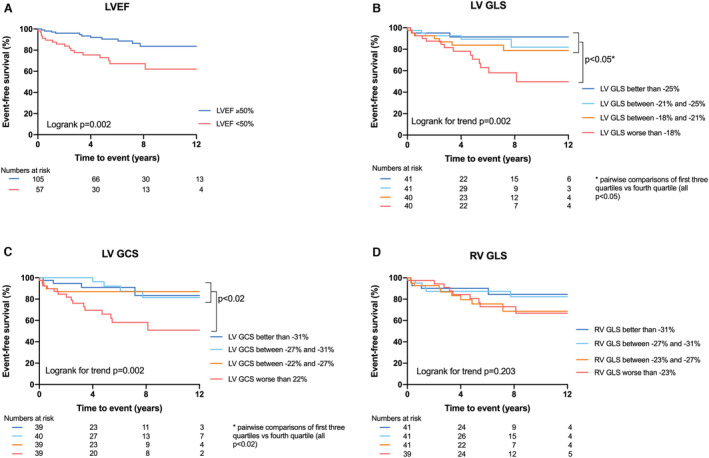
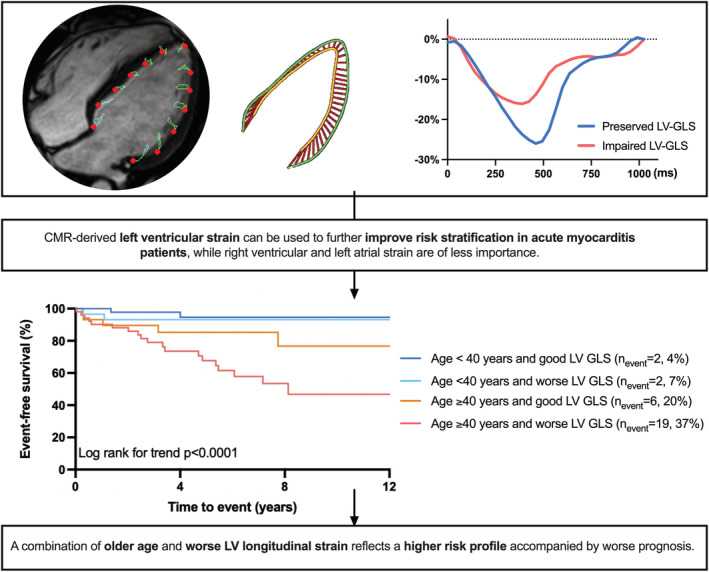
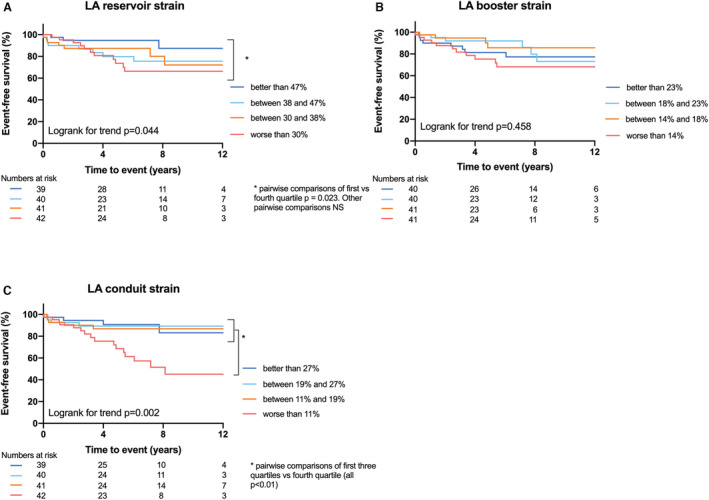
Background Late gadolinium enhancement and left ventricular (LV) ejection fraction on cardiovascular magnetic resonance (CMR) are prognostic markers, but their predictive value for incident heart failure or life-threatening arrhythmias in acute myocarditis patients is limited. CMR-derived feature tracking provides a more sensitive analysis of myocardial function and may improve risk stratification in myocarditis. In this study, the prognostic value of LV, right ventricular, and left atrial strain in acute myocarditis patients is evaluated. Methods and Results In this multicenter retrospective study, patients with CMR-proven acute myocarditis were included. The primary end point was occurrence of major adverse cardiovascular events: all-cause mortality, heart transplantation, heart failure hospitalizations, and life threatening arrhythmias. LV global longitudinal strain, global circumferential strain and global radial strain, right ventricular-global longitudinal strain and left atrial strain were measured. Unadjusted and adjusted cox proportional hazard regression analysis were performed. In total, 162 CMR-proven myocarditis patients were included (41 ± 17 years, 75% men). Mean LV ejection fraction was 51 ± 12%, and 144 (89%) patients had presence of late gadolinium enhancement. Major adverse cardiovascular events occurred in 29 (18%) patients during a follow-up of 5.5 (2.2-8.3) years. All LV strain parameters were independent predictors of outcome beyond clinical features, LV ejection fraction and late gadolinium enhancement (LV-global longitudinal strain: hazard ratio [HR] 1.07, =0.02; LV-global circumferential strain: HR 1.15, =0.02; LV-global radial strain: HR 0.98, =0.03), but right ventricular or left atrial strain did not predict outcome. Conclusions CMR-derived LV strain analysis provides independent prognostic value on top of clinical parameters, LV ejection fraction and late gadolinium enhancement in acute myocarditis patients, while left atrial and right ventricular strain seem to be of less importance.
心血管磁共振(CMR)上的晚期钆增强和左心室(LV)射血分数是预后标志物,但它们对急性心肌炎患者心力衰竭或危及生命的心律失常事件的预测价值有限。CMR 衍生的应变分析提供了一种更敏感的心肌功能分析方法,可能改善心肌炎的风险分层。在本研究中,评估了 LV、右心室和左心房应变在急性心肌炎患者中的预后价值。
这是一项多中心回顾性研究,纳入了 CMR 证实的急性心肌炎患者。主要终点是主要不良心血管事件的发生:全因死亡率、心脏移植、心力衰竭住院和危及生命的心律失常。测量 LV 整体纵向应变、整体周向应变和整体径向应变、右心室整体纵向应变和左心房应变。进行了未经调整和调整后的 Cox 比例风险回归分析。共纳入 162 例 CMR 证实的心肌炎患者(41±17 岁,75%为男性)。平均 LV 射血分数为 51±12%,144 例(89%)患者存在晚期钆增强。在 5.5(2.2-8.3)年的随访期间,29 例(18%)患者发生主要不良心血管事件。所有 LV 应变参数均为临床特征、LV 射血分数和晚期钆增强之外的独立预后预测因素(LV 整体纵向应变:危险比[HR]1.07,=0.02;LV 整体周向应变:HR 1.15,=0.02;LV 整体径向应变:HR 0.98,=0.03),但右心室或左心房应变不能预测结局。
CMR 衍生的 LV 应变分析在急性心肌炎患者中,除了临床参数、LV 射血分数和晚期钆增强外,还提供了独立的预后价值,而左心房和右心室应变的重要性较低。