Department of Mental Health, AULSS3 Serenissima, Venice, Italy.
Department of Rehabilitation Sciences, KU Leuven University, Leuven, Belgium.
Mol Psychiatry. 2023 Jan;28(1):369-390. doi: 10.1038/s41380-022-01770-w. Epub 2022 Sep 22.
People with mood disorders have increased risk of comorbid medical diseases versus the general population. It is paramount to identify interventions to improve physical health in this population.
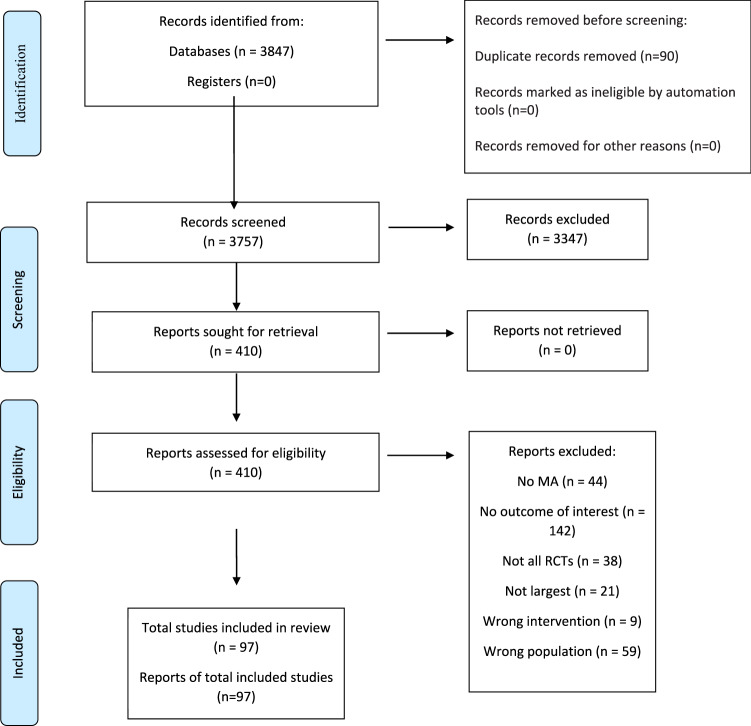
Umbrella review of meta-analyses of randomised controlled trials (RCTs) on pharmacological/non-pharmacological interventions for physical health outcomes/intolerability-related discontinuation in mood disorders (any age).
Ninety-seven meta-analyses were included. Among youths, against placebo, in depression, antidepressants/antipsychotics had higher discontinuation rates; in bipolar depression, olanzapine+fluoxetine worsened total cholesterol (TC)/triglycerides/weight gain (WG) (large ES). In adults with bipolar disorder, olanzapine worsened HbA1c/TC/WG (moderate/large ES); asenapine increased fasting glucose (small ES); quetiapine/cariprazine/risperidone induced WG (small/moderate ES). In bipolar depression, lurasidone was metabolically neutral. In depression, psychological interventions improved physical health-related quality of life (PHQoL) (small ES), fasting glucose/HbA1c (medium/large ES); SSRIs improved fasting glucose/HbA1c, readmission for coronary disease, pain (small ES); quetiapine/aripiprazole/olanzapine induced WG (small to large ES). Exercise improved cardiorespiratory fitness (moderate ES). In the elderly, fluoxetine yielded more detrimental cardiovascular effects than sertraline/escitalopram (large ES); antidepressants were neutral on exercise tolerance and PHQoL. In mixed age groups, in bipolar disorder aripiprazole was metabolically neutral; in depression, SSRIs lowered blood pressure versus placebo and serotonin-noradrenaline reuptake inhibitors (small ES); brexpiprazole augmentation caused WG and was less tolerated (small ES); exercise improved PHQoL (moderate ES).
Some interventions (psychological therapies, exercise and SSRIs) improve certain physical health outcomes in mood disorders, few are neutral, but various pharmacological interventions are associated with negative effects. Evidence from this umbrella review has limitations, should consider evidence from other disorders and should be integrated with recent evidence from individual RCTs, and observational evidence. Effective treatments with either beneficial or physically neutral profiles should be prioritized.
与普通人群相比,患有心境障碍的人群合并患有多种医学疾病的风险增加。当务之急是确定改善该人群身体健康的干预措施。
对心境障碍(任何年龄)患者中药物/非药物干预对身体健康结果/不耐受相关停药的随机对照试验(RCT)的荟萃分析进行伞式综述。
纳入了 97 项荟萃分析。在青少年中,与安慰剂相比,抗抑郁药/抗精神病药在治疗抑郁症时停药率更高;在双相抑郁症中,奥氮平+氟西汀会加重总胆固醇(TC)/甘油三酯(TG)/体重增加(WG)(大 ES)。在成人双相障碍中,奥氮平会加重糖化血红蛋白(HbA1c)/TC/WG(中/大 ES);阿那曲唑会增加空腹血糖(小 ES);喹硫平/卡利培嗪/利培酮会导致 WG(小/中 ES)。在双相抑郁症中,鲁拉西酮对代谢是中性的。在抑郁症中,心理干预可改善身体健康相关生活质量(PHQoL)(小 ES)、空腹血糖/HbA1c(中/大 ES);SSRIs 可改善空腹血糖/HbA1c、因冠心病再入院、疼痛(小 ES);喹硫平/阿立哌唑/奥氮平导致 WG(小至大 ES)。运动可改善心肺适应性(中 ES)。在老年人中,氟西汀对心血管的影响比舍曲林/艾司西酞普兰更不利(大 ES);抗抑郁药对运动耐量和 PHQoL 无影响。在混合年龄组中,在双相障碍中阿立哌唑对代谢是中性的;在抑郁症中,SSRIs 降低血压优于安慰剂和 5-羟色胺去甲肾上腺素再摄取抑制剂(小 ES);布瑞哌唑增效导致 WG 且耐受性差(小 ES);运动可改善 PHQoL(中 ES)。
一些干预措施(心理疗法、运动和 SSRIs)可改善心境障碍患者的某些身体健康结果,少数是中性的,但各种药物干预与不良影响有关。本伞式综述的证据存在局限性,应考虑其他疾病的证据,并应与最近的个体 RCT 观察性证据进行整合。具有有益或对身体无影响的有效治疗方法应优先考虑。