Kołodziejska Katarzyna, Witowski Jan, Tylec Piotr, Grochowska Anna, Przytuła Natalia, Lis Maciej, Pędziwiatr Michał, Rubinkiewicz Mateusz
Department of Medical Education, Faculty of Medicine, Jagiellonian University Medical College, 30-688 Kraków, Poland.
Department of Radiology, New York University Grossman School of Medicine, New York, NY 10016, USA.
J Clin Med. 2022 Sep 13;11(18):5365. doi: 10.3390/jcm11185365.
As the number of elderly patients requiring surgical intervention rises, it is believed that frailty syndrome has a greater impact on perioperative course than on chronological age. The aim of this study was to evaluate the efficacy of various imaging features for frailty assessment in patients undergoing emergency laparotomy.
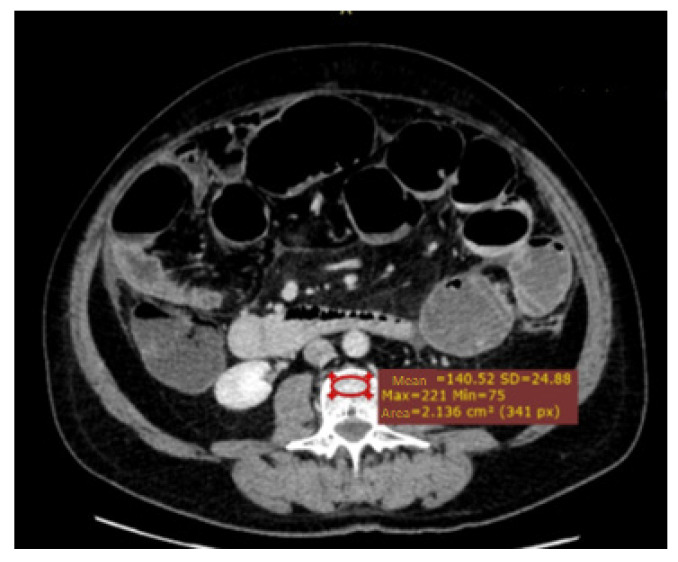
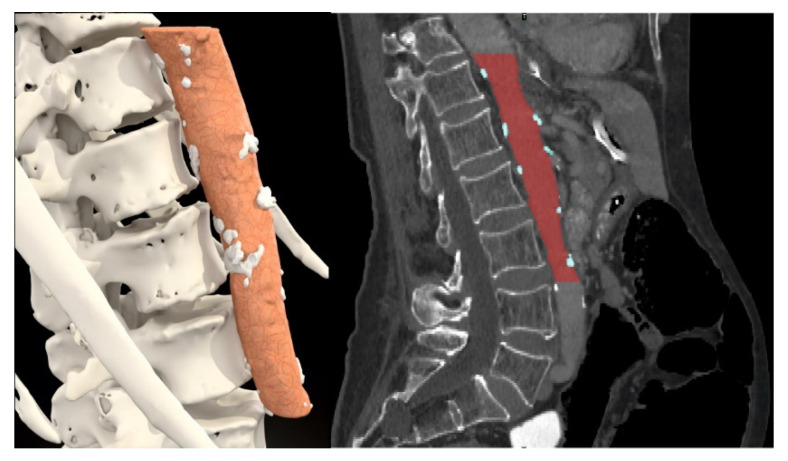
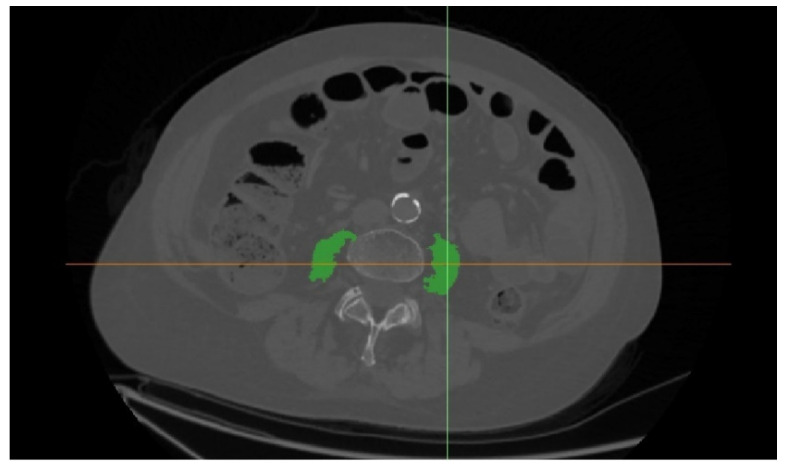
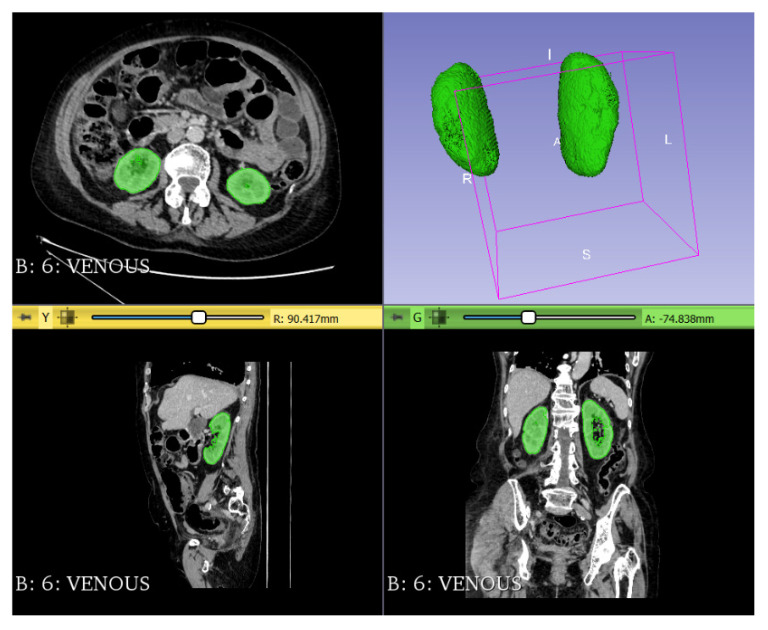
The study included all patients that qualified for emergency surgery with preoperative CT scans between 2016 and 2020 in the Second Department of General Surgery. Multiple trauma patients were excluded from the analysis. The modified frailty index and brief geriatric assessment were used in the analysis. CT images were reviewed for the assessment of osteopenia, sarcopenia, sarcopenic obesity, renal volume and abdominal aorta calcification rate.
A total of 261 patients were included in the analysis. Multivariate logistic regression identified every next ASA class (OR: 4.161, 95%CI: 1.672-10.355, = 0.002), intraoperative adverse events (OR: 12.397, 95%CI: 2.166-70.969, = 0.005) and osteopenia (OR: 4.213, 95%CI: 1.235-14.367, = 0.022) as a risk factor for 30-day mortality. Our study showed that every next ASA class (OR: 1.952, 95%Cl: 1.171-3.256, = 0.010) and every point of the BGA score (OR: 1.496, 95%Cl: 1.110-2.016, = 0.008) are risk factors for major complications.
Osteopenia was the best parameter for perioperative mortality risk stratification in patients undergoing emergency surgical intervention. Sarcopenia (measured as psoas muscle area), sarcopenic obesity, aortic calcifications and mean kidney volume do not predict poor outcomes in those patients. None of the radiological markers appeared to be useful for the prediction of perioperative morbidity.
随着需要手术干预的老年患者数量的增加,人们认为衰弱综合征对围手术期过程的影响大于实际年龄。本研究的目的是评估各种影像学特征在接受急诊剖腹手术患者中进行衰弱评估的有效性。
该研究纳入了2016年至2020年在普通外科第二科室接受术前CT扫描且符合急诊手术条件的所有患者。分析中排除了多发伤患者。分析中使用了改良衰弱指数和简易老年评估。对CT图像进行评估以确定骨质减少、肌肉减少症、肌肉减少性肥胖、肾体积和腹主动脉钙化率。
共有261例患者纳入分析。多因素逻辑回归确定每升高一级美国麻醉医师协会(ASA)分级(比值比:4.161,95%置信区间:1.672 - 10.355,P = 0.002)、术中不良事件(比值比:12.397,95%置信区间:2.166 - 70.969,P = 0.005)和骨质减少(比值比:4.213,95%置信区间:1.235 - 14.367,P = 0.022)是30天死亡率的危险因素。我们的研究表明,每升高一级ASA分级(比值比:1.952,95%置信区间:1.171 - 3.256,P = 0.010)和简易老年评估(BGA)评分的每一分(比值比:1.496,95%置信区间:1.110 - 2.016,P = 0.008)是主要并发症的危险因素。
骨质减少是接受急诊手术干预患者围手术期死亡风险分层的最佳参数。肌肉减少症(以腰大肌面积衡量)、肌肉减少性肥胖、主动脉钙化和平均肾体积不能预测这些患者的不良结局。没有任何影像学标志物似乎对围手术期发病率的预测有用。