Chaudhry Isha, Shafiq Mahham, Teo Irene, Ozdemir Semra, Malhotra Chetna
Lien Centre for Palliative Care, Duke-NUS Medical School, Singapore, Singapore.
Health Services and System Research, Duke-NUS Medical School, Singapore, Singapore.
J Pain Res. 2022 Sep 16;15:2949-2956. doi: 10.2147/JPR.S375874. eCollection 2022.
Despite medical advancements, pain is a major source of suffering at the end of life for patients with a solid metastatic cancer. We aimed to assess the trajectory of pain prevalence, severity, interference, and inadequacy of analgesia during the last year of life.
We analysed data from the last year of life of 345 decedents from a prospective cohort study of 600 patients with a solid metastatic cancer in Singapore. Patients were surveyed every 3 months and their pain outcomes (prevalence, severity, and interference) and inadequacy of analgesia were analysed. We used mixed-effects regressions to assess the association of pain outcomes with patients' time from death, demographics, and planned or unplanned hospitalisations.
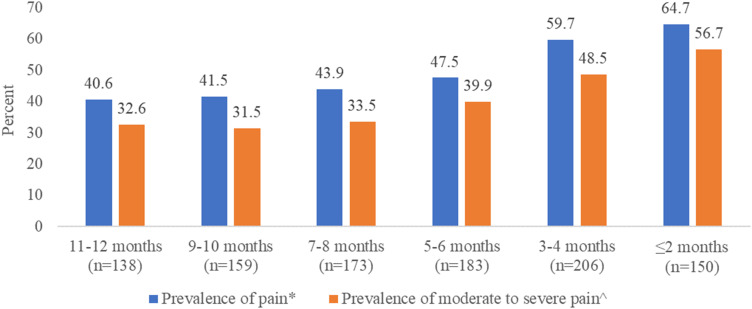
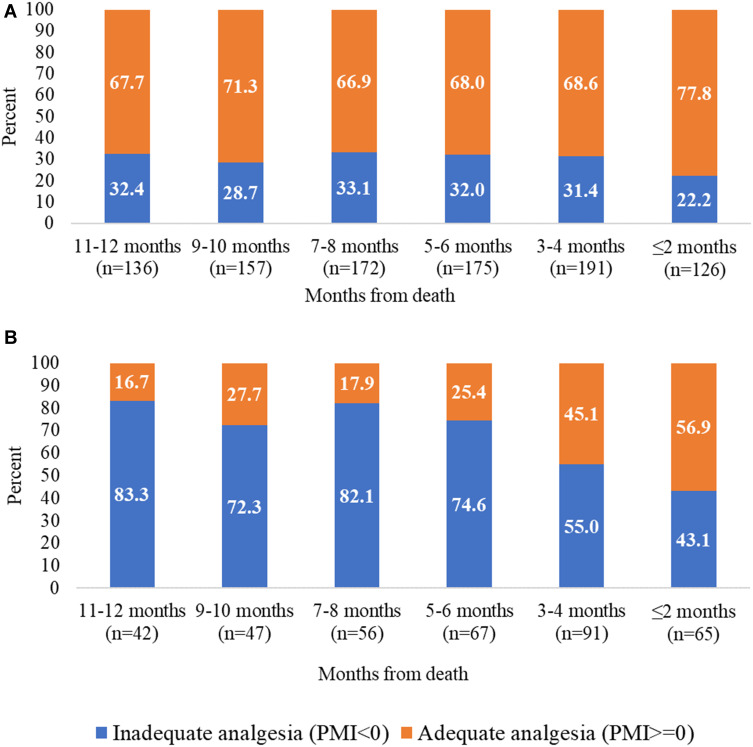
Prevalence of pain was higher in the last 2 months (65%) compared to 11 to 12 months (41%) before death. Pain severity and interference scores (mean ± SD) were also higher in the last month (severity: 2.5±2.6; interference: 2.6±3.0) compared to 12 months before death (severity: 1.4±2.0; interference: 1.4±2.0). At any time during the last year of life, 38% of the patients were prescribed non-steroidal anti-inflammatory drugs, 11% were prescribed weak-opioids and 29% were prescribed strong opioids. These analgesics were prescribed through either oral, topical or injectable route. Pain outcomes were significantly worse (p-value<0.05) for younger patients, those with higher education, and more financial difficulties, while interference was higher after an unplanned hospitalisation in the last month. Females reported higher pain severity score during their last year of life compared to males. For patients reporting moderate to severe pain, inadequacy of analgesia was lower in the last 2 months (43%) compared to 11 to 12 months before death (83%).
Findings highlight the need for greater attention in monitoring and treatment of pain even earlier in the disease trajectory, and increased attention to patients discharged from an unplanned hospitalisation.
尽管医学不断进步,但对于患有实体转移性癌症的患者而言,疼痛仍是其生命末期痛苦的主要来源。我们旨在评估生命最后一年中疼痛发生率、严重程度、干扰程度以及镇痛不足情况的变化轨迹。
我们分析了来自新加坡一项针对600例实体转移性癌症患者的前瞻性队列研究中345例死者生命最后一年的数据。每3个月对患者进行一次调查,并分析他们的疼痛结局(发生率、严重程度和干扰程度)以及镇痛不足情况。我们使用混合效应回归来评估疼痛结局与患者距死亡时间、人口统计学特征以及计划内或计划外住院之间的关联。
与死亡前11至12个月(41%)相比,最后2个月的疼痛发生率更高(65%)。与死亡前12个月相比,最后一个月的疼痛严重程度和干扰评分(均值±标准差)也更高(严重程度:2.5±2.6;干扰程度:2.6±3.0),而死亡前12个月时严重程度为1.4±2.0;干扰程度为1.4±2.0。在生命的最后一年中的任何时候,38%的患者被开具了非甾体类抗炎药,11%的患者被开具了弱阿片类药物,29%的患者被开具了强阿片类药物。这些镇痛药通过口服、局部用药或注射途径给药。年轻患者、受过高等教育的患者以及经济困难较多的患者的疼痛结局明显更差(p值<0.05),而在最后一个月计划外住院后干扰程度更高。女性在生命最后一年报告的疼痛严重程度评分高于男性。对于报告中度至重度疼痛的患者,与死亡前11至12个月(83%)相比,最后2个月的镇痛不足情况更低(43%)。
研究结果凸显了在疾病进程中更早地对疼痛进行监测和治疗的必要性,以及对计划外住院出院患者给予更多关注。