Department of Oncology, The Fifth Medical Center of PLA General Hospital, Beijing, China.
Department of Oncology, The Seventh Medical Center of PLA General Hospital, Beijing, China.
Front Immunol. 2022 Sep 9;13:975246. doi: 10.3389/fimmu.2022.975246. eCollection 2022.
The efficacy of immune checkpoint inhibitors (ICIs) in pretreated -mutated non-small cell lung cancer (NSCLC) patients is controversial. We conducted this multicenter retrospective study to examine the efficacy of ICIs in a real world setting.
We collected 116 consecutive NSCLC patients with sensitive mutations who received ICIs alone or in combination after failure to respond to EGFR tyrosine kinase inhibitors (EGFR-TKIs), and 99 patients were included for final analysis. The impacts of ICIs on the patients' objective response rate (ORR), disease control rate (DCR), progression-free survival (PFS), and overall survival (OS) were assessed. The relationships between outcomes and clinical characteristics were analyzed.
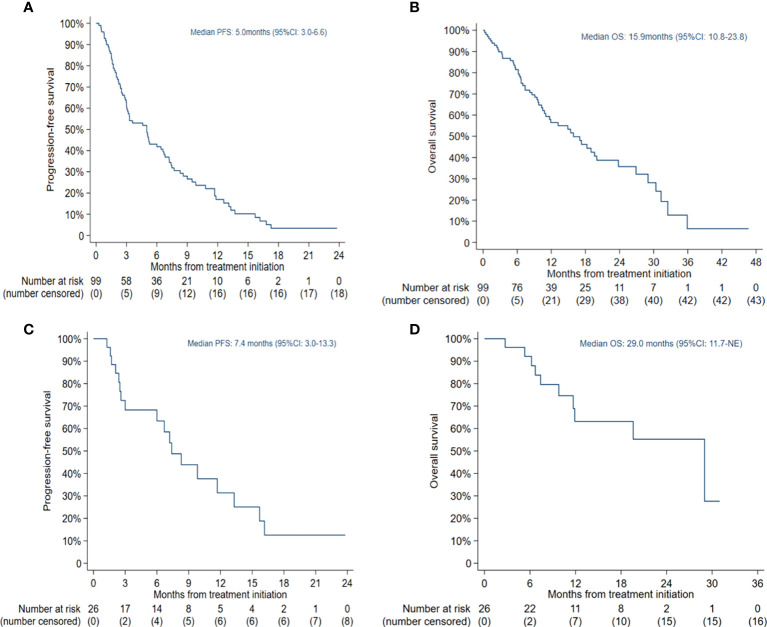
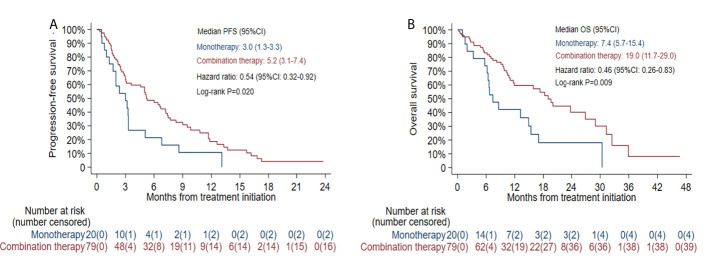
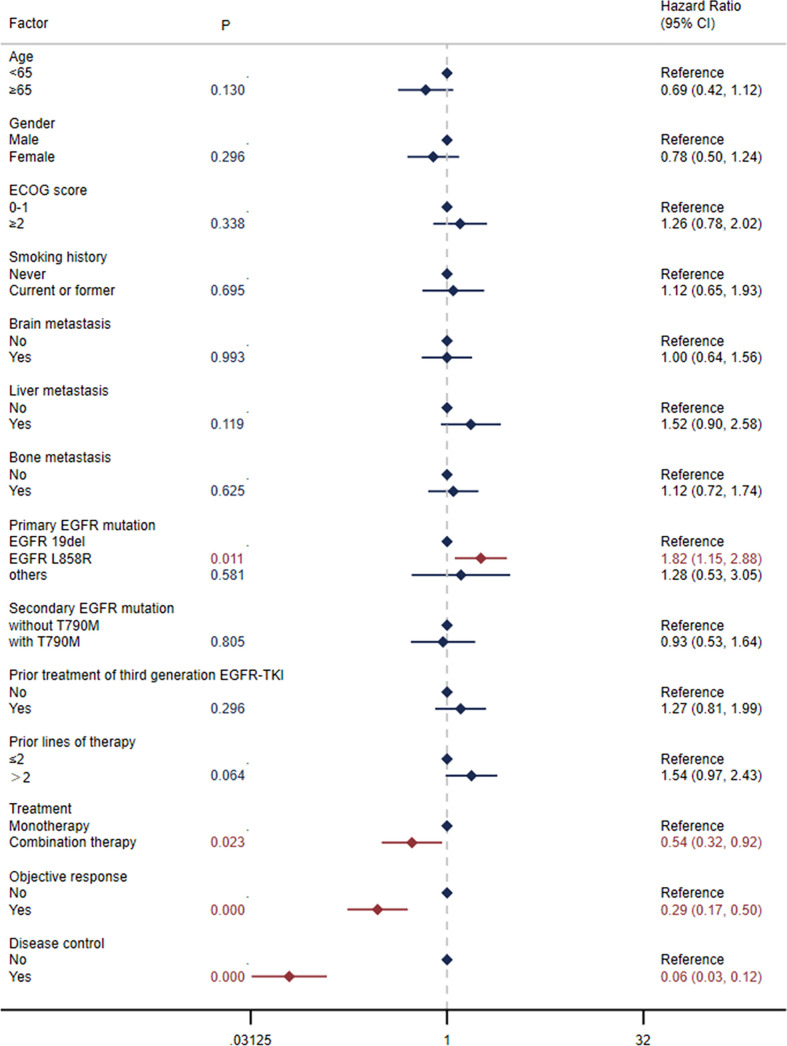
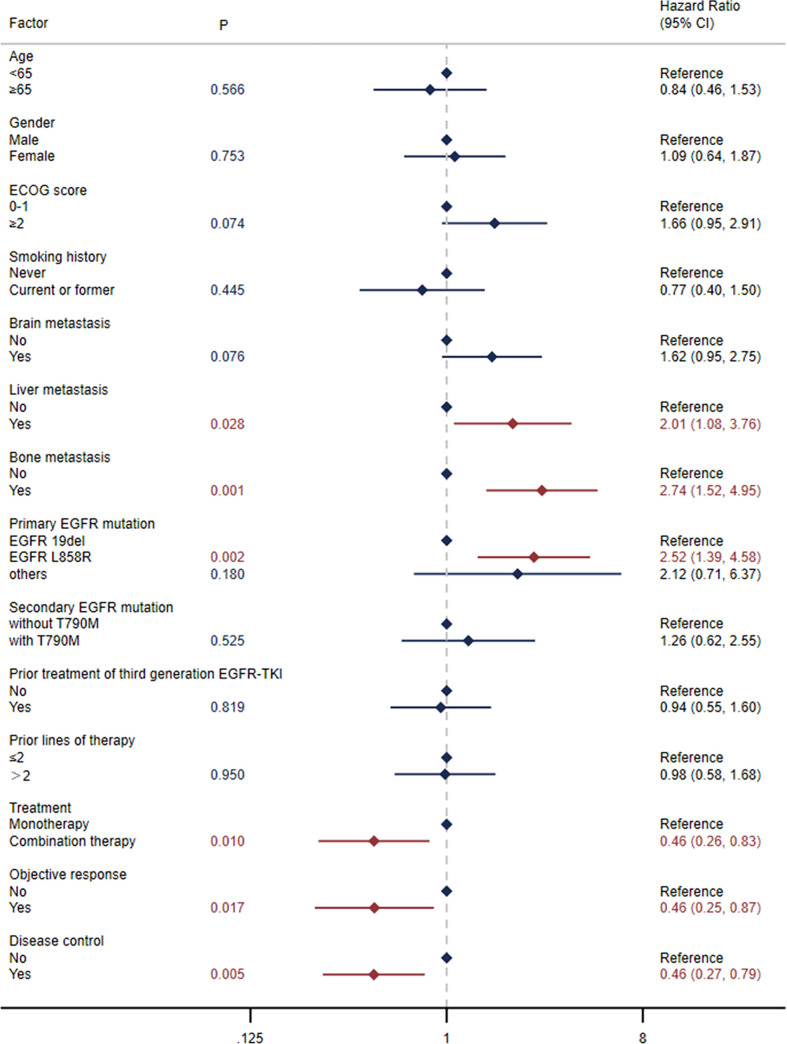
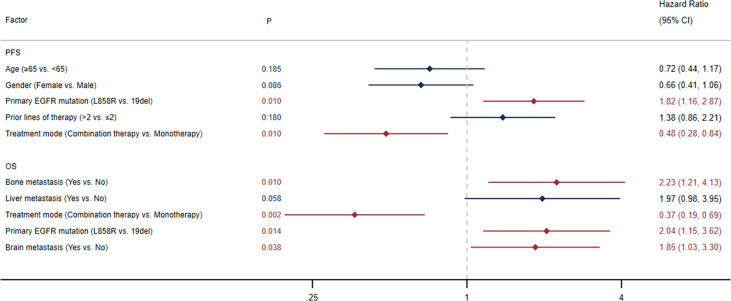
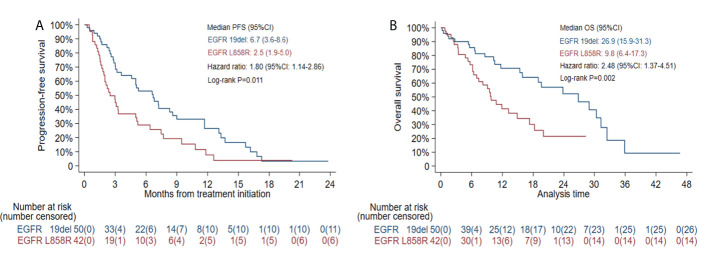
The ORR in patients with target lesions was 31.25% (95% CI: 22.18-41.52), and the DCR in all patients was 65.66% (95% CI: 55.44-74.91). The overall median PFS was 5.0 months (95% CI: 3.0-6.6), and the median OS was 15.9 months (95% CI: 10.8-23.8). The outcomes were better in patients receiving combination therapy with ECOG scores of 0-1 and no more than 2 lines of prior therapy, with a median PFS of 7.4 months (95% CI: 3.0-13.3) and a median OS of 29.0 months (95% CI: 11.7-NE). Primary mutation type and treatment mode were found to have a notable impact on clinical outcomes. Both median PFS and OS in patients with L858R mutation were significantly shorter than those in patients with exon 19 deletion (19del) (PFS: 2.5 versus 6.7 months, HR: 1.80, log-rank =0.011; OS: 9.8 versus 26.9 months, HR: 2.48, log-rank =0.002). Patients receiving combination therapy had notably longer median PFS and OS than those receiving monotherapy (PFS: 5.2 versus 3.0 months, HR: 0.54, log-rank =0.020; OS: 19.0 versus 7.4 months, HR: 0.46, log-rank =0.009).
Our study suggests that ICI-based combination therapy is a potential strategy for -mutated NSCLC patients after EGFR-TKI failure. The efficacy may differ according to subtypes.
免疫检查点抑制剂(ICIs)在预处理-突变非小细胞肺癌(NSCLC)患者中的疗效存在争议。我们进行了这项多中心回顾性研究,以在真实环境中检查 ICI 的疗效。
我们收集了 116 例接受 EGFR 酪氨酸激酶抑制剂(EGFR-TKIs)治疗失败后单独或联合接受 ICI 治疗的敏感突变 NSCLC 患者,其中 99 例患者纳入最终分析。评估 ICI 对患者客观缓解率(ORR)、疾病控制率(DCR)、无进展生存期(PFS)和总生存期(OS)的影响。分析了结果与临床特征之间的关系。
有靶病灶患者的 ORR 为 31.25%(95%CI:22.18-41.52),所有患者的 DCR 为 65.66%(95%CI:55.44-74.91)。总体中位 PFS 为 5.0 个月(95%CI:3.0-6.6),中位 OS 为 15.9 个月(95%CI:10.8-23.8)。在 ECOG 评分为 0-1 分且接受治疗线数不超过 2 线的患者中,联合治疗的结局更好,中位 PFS 为 7.4 个月(95%CI:3.0-13.3),中位 OS 为 29.0 个月(95%CI:11.7-NE)。主要 突变类型和治疗方式对临床结局有显著影响。L858R 突变患者的中位 PFS 和 OS 均显著短于 19 号外显子缺失(19del)患者(PFS:2.5 与 6.7 个月,HR:1.80,对数秩检验=0.011;OS:9.8 与 26.9 个月,HR:2.48,对数秩检验=0.002)。联合治疗组的中位 PFS 和 OS 均显著长于单药治疗组(PFS:5.2 与 3.0 个月,HR:0.54,对数秩检验=0.020;OS:19.0 与 7.4 个月,HR:0.46,对数秩检验=0.009)。
本研究表明,ICI 联合治疗可能是 EGFR-TKI 治疗失败后的-突变 NSCLC 患者的一种潜在策略。疗效可能因 亚型而异。