Early Detection, Prevention and Infections Branch, International Agency for Research on Cancer, World Health Organization (IARC/WHO), Lyon, France.
Early Detection, Prevention and Infections Branch, International Agency for Research on Cancer, World Health Organization (IARC/WHO), Lyon, France.
Lancet Oncol. 2022 Nov;23(11):1419-1429. doi: 10.1016/S1470-2045(22)00543-5. Epub 2022 Sep 26.
Despite the high burden of cervical cancer, access to preventive measures remains low in India. A single-dose immunisation schedule could facilitate the scale-up of human papillomavirus (HPV) vaccination, contributing to global elimination of cervical cancer. We projected the effect of single-dose quadrivalent HPV vaccination in India in comparison with no vaccination or to a two-dose schedule.
In this modelling study, we adapted an HPV transmission model (EpiMetHeos) to Indian data on sexual behaviour (from the Demographic and Health Survey and the Indian National AIDS Control Organisation), HPV prevalence data (from two local surveys, from the states of Tamil Nadu and West Bengal), and cervical cancer incidence data (from Cancer Incidence in Five Continents for the period 2008-12 [volume XI], and the Indian National Centre for Disease Informatics and Research for the period 2012-16). Using the model, we projected the nationwide and state-specific effect of HPV vaccination on HPV prevalence and cervical cancer incidence, and lifetime risk of cervical cancer, for 100 years after the introduction of vaccination or in the first 50 vaccinated birth cohorts. Projections were derived under a two-dose vaccination scenario assuming life-long protection and under a single-dose vaccination scenario with protection duration assumptions derived from International Agency for Research on Cancer (IARC) India vaccine trial data, in combination with different vaccination coverages and catch-up vaccination age ranges. We used two thresholds to define cervical cancer elimination: an age-standardised incidence rate of less than 4 cases per 100 000 woman-years, and standardised lifetime risk of less than 250 cases per 100 000 women born.
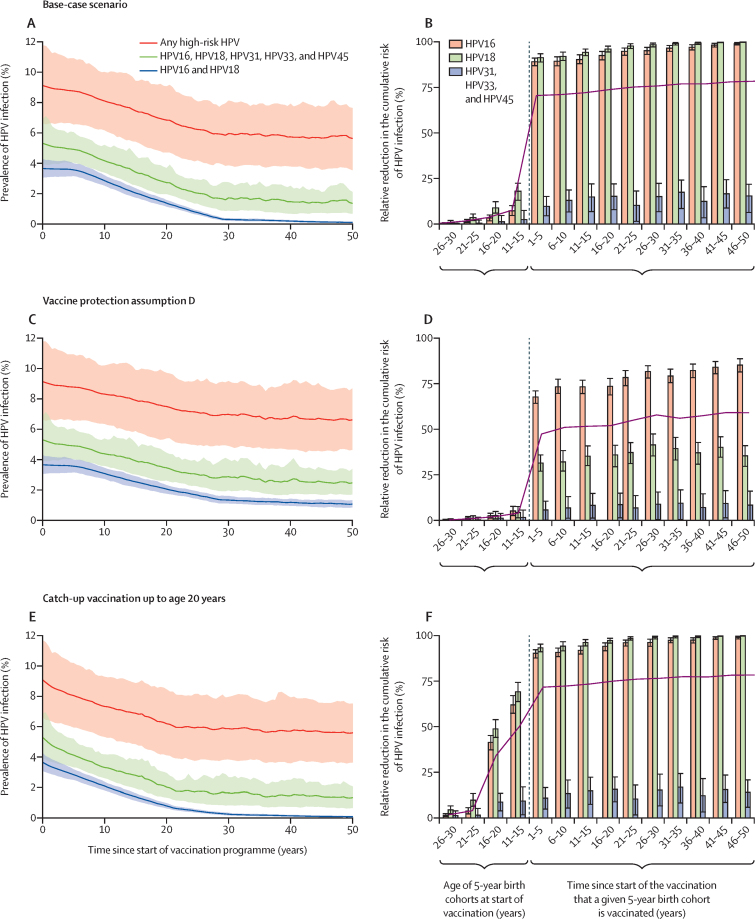
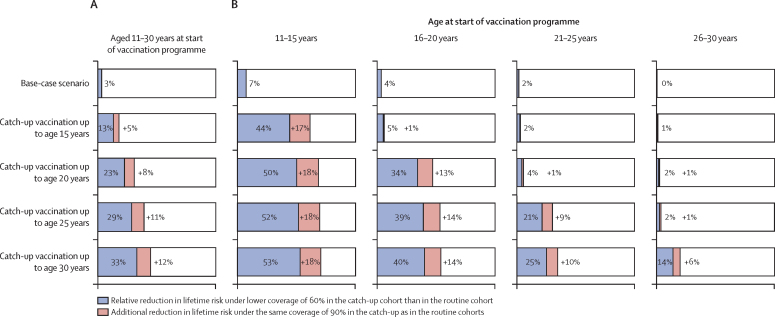
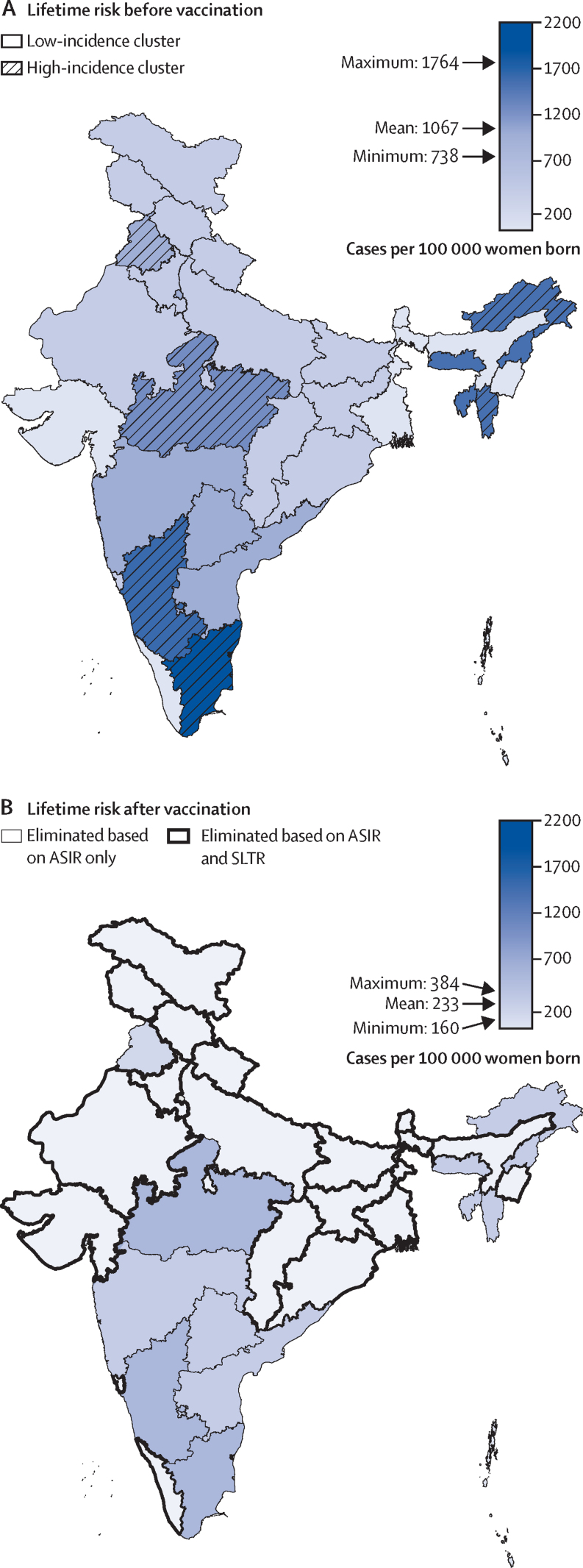
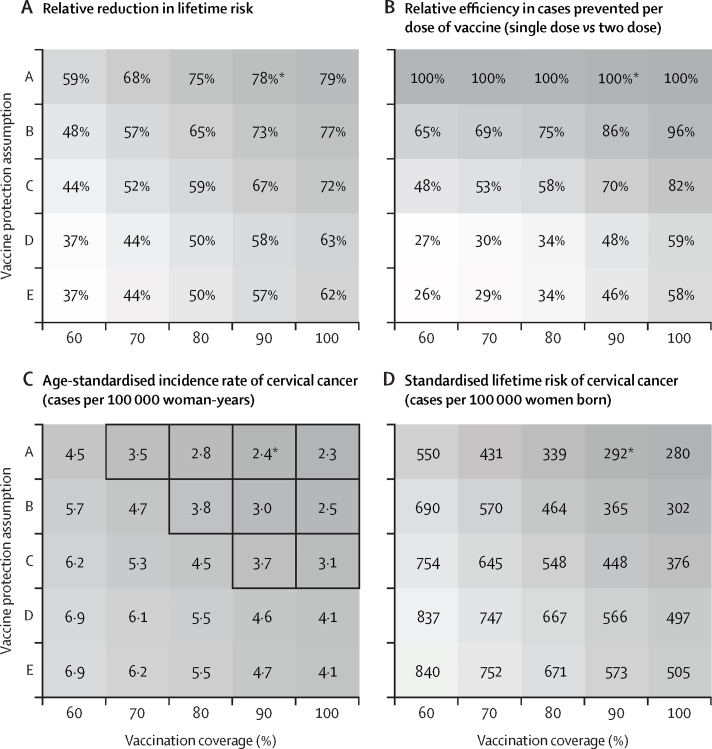
Assuming vaccination in girls aged 10 years, with 90% coverage, and life-long protection by two-dose or single-dose schedule, HPV vaccination could reduce the prevalence of HPV16 and HPV18 infection by 97% (80% UI 96-99) in 50 years, and the lifetime risk of cervical cancer by 71-78% from 1067 cases per 100 000 women born under a no vaccination scenario to 311 (80% UI 284-339) cases per 100 000 women born in the short term and 233 (219-252) cases per 100 000 women born in the long term in vaccinated cohorts. Under this scenario, we projected that the age-standardised incidence rate threshold for elimination could be met across India (range across Indian states: 1·6 cases [80% UI 1·5-1·7] to 4·0 cases [3·8-4·4] per 100 000 woman-years), while the complementary threshold based on standardised lifetime risk was attainable in 17 (68%) of 25 states, but not nationwide (range across Indian states: 207 cases [80% UI 194-223] to 477 cases [447-514] per 100 000 women born). Under the considered assumptions of waning vaccine protection, single-dose vaccination was projected to have a 21-100% higher per-dose efficiency than two-dose vaccination. Single-dose vaccination with catch-up for girls and women aged 11-20 years was more impactful than two-dose vaccination without catch-up, with reduction of 39-65% versus 38% in lifetime risk of cervical cancer across the ten catch-up birth cohorts and the first ten routine vaccination birth cohorts.
Our evidence-based projections suggest that scaling up cervical cancer prevention through single-dose HPV vaccination could substantially reduce cervical cancer burden in India.
The Bill & Melinda Gates Foundation.
尽管宫颈癌负担沉重,但印度获得预防措施的机会仍然很低。单剂免疫接种计划可以促进人乳头瘤病毒(HPV)疫苗的推广,有助于全球消除宫颈癌。我们预测了在印度与不接种疫苗或两剂接种计划相比,单剂四价 HPV 疫苗接种的效果。
在这项建模研究中,我们根据印度性传播行为的数据(来自人口与健康调查和印度国家艾滋病控制组织)、HPV 流行率数据(来自两个地方调查,来自泰米尔纳德邦和西孟加拉邦)和宫颈癌发病率数据(来自 2008-12 年的《五大洲癌症发病率》第 11 卷,以及 2012-16 年的印度国家疾病信息和研究中心),对 HPV 传播模型(EpiMetHeos)进行了调整。利用该模型,我们预测了 HPV 疫苗接种在 100 年内对 HPV 流行率和宫颈癌发病率以及宫颈癌终生风险的全国和州特定影响,以及在引入疫苗接种后的前 50 个接种出生队列中。假设终生保护,在两剂接种方案下,根据假设的国际癌症研究机构(IARC)印度疫苗试验数据和不同的疫苗覆盖率和补种年龄范围得出的保护持续时间,在单剂接种方案下进行了预测。我们使用两个阈值来定义宫颈癌消除:年龄标准化发病率低于每 10 万女性 4 例,以及标准终生风险低于每 10 万名出生女性 250 例。
假设在 10 岁女孩中接种疫苗,覆盖率为 90%,两剂或单剂方案终生保护,HPV 疫苗接种可在 50 年内将 HPV16 和 HPV18 感染的流行率降低 97%(80%UI 96-99),从无疫苗接种情况下每 10 万名出生女性 1067 例宫颈癌终生风险降低 71-78%,在短期内每 10 万名出生女性 311 例(80%UI 284-339),在长期每 10 万名出生女性 233 例(219-252)。在此方案下,我们预测消除的年龄标准化发病率阈值可以在印度全国范围内达到(印度各州范围:1.6 例[80%UI 1.5-1.7]至 4.0 例[3.8-4.4]每 10 万女性),而基于标准终生风险的补充阈值在 25 个州中的 17 个(68%)州是可以达到的,但在全国范围内是无法达到的(印度各州范围:207 例[80%UI 194-223]至 477 例[447-514]每 10 万名出生女性)。在所考虑的疫苗保护效力下降的假设下,单剂疫苗接种的每剂效率预计比两剂疫苗接种高 21-100%。对于 11-20 岁的女孩和妇女进行单剂疫苗接种和补种比两剂疫苗接种不补种更有效果,在 10 个补种出生队列和前 10 个常规接种出生队列中,宫颈癌终生风险降低 39-65%,而不是 38%。
我们基于证据的预测表明,通过单剂 HPV 疫苗接种来扩大宫颈癌预防工作,可以大大减轻印度的宫颈癌负担。
比尔和梅琳达·盖茨基金会。