Department of Surgery, Kuma Hospital, 8-2-35, Shimoyamate-dori, Kobe, Hyogo, 650-0011, Japan.
Department of Head and Neck Surgery, Kuma Hospital, Kobe, Hyogo, 650-0011, Japan.
World J Surg. 2023 Feb;47(2):392-401. doi: 10.1007/s00268-022-06770-z. Epub 2022 Oct 2.
Active surveillance (AS) of low-risk papillary thyroid microcarcinoma (PTMC) was initiated at Kuma Hospital in 1993 and is gradually spreading worldwide. We assessed the effect of thyroid-stimulating hormone (TSH) levels on PTMC enlargement in patients on AS.
We enrolled 2705 patients with cytologically diagnosed PTMC who had undergone AS between January 2005 and July 2019. Patients with Graves disease were excluded. The median AS period was 5.5 years (range 1.0-15.7 years). Tumor enlargement was defined as a size increase ≥3 mm. Chi-square test, Kaplan-Meier method, log-rank test, Cox proportional hazard, and logistic regression were used to compare variables.
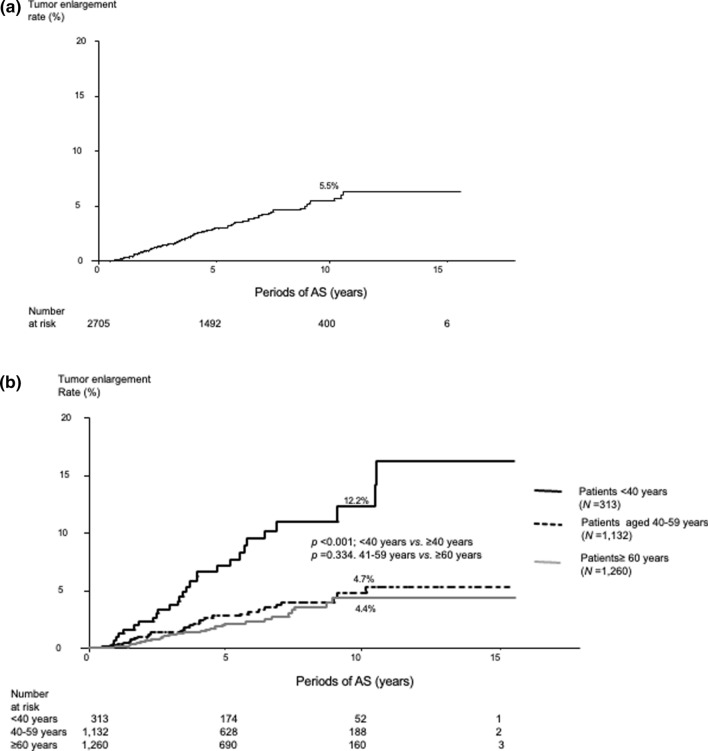
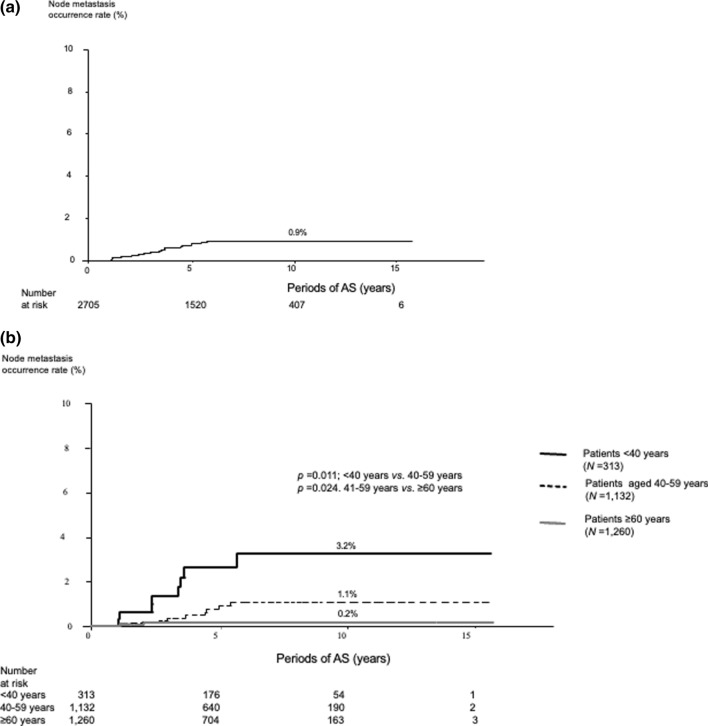
Ninety-two patients (3.4%) experienced tumor enlargement; the 5-, 10-, and 15-year enlargement rates were 3.0%, 5.5%, and 6.2%, respectively. Young age (<40 years, p < 0.001), large tumor size (≥9 mm, p = 0.017), and high detailed TSH score (≥3, higher than the lower normal limit, p = 0.011) were significant factors relating to tumor enlargement in the multivariate analysis. In a subset of patients aged <40 years, a low detailed TSH score (<3) was an independent factor against tumor enlargement (p = 0.039). Only 22 patients (0.8%) experienced novel lymph node metastasis; the 5-, 10-, and 15-year node metastasis rates were very low, at 0.9%, 1.1%, and 1.1%, respectively.
Young patients with PTMC are more likely to experience tumor growth. Mild TSH suppression to achieve a low normal range may prevent carcinoma enlargement; however, prospective studies are needed to draw more reliable conclusions.
1993 年熊本大学医院开始对低危型甲状腺微小乳头状癌(PTMC)进行主动监测(AS),该方法逐渐在全球范围内得到推广。本研究评估了促甲状腺激素(TSH)水平对 AS 患者 PTMC 增大的影响。
本研究纳入了 2005 年 1 月至 2019 年 7 月间接受 AS 的 2705 例细胞学诊断为 PTMC 的患者。排除了 Graves 病患者。AS 中位时间为 5.5 年(1.0-15.7 年)。肿瘤增大定义为大小增加≥3mm。采用卡方检验、Kaplan-Meier 法、log-rank 检验、Cox 比例风险和 logistic 回归分析比较变量。
92 例(3.4%)患者发生肿瘤增大;5、10 和 15 年的增大率分别为 3.0%、5.5%和 6.2%。多因素分析显示,年龄较小(<40 岁,p<0.001)、肿瘤较大(≥9mm,p=0.017)和详细 TSH 评分较高(≥3,高于正常下限,p=0.011)是肿瘤增大的显著相关因素。在年龄<40 岁的患者亚组中,低详细 TSH 评分(<3)是肿瘤增大的独立因素(p=0.039)。仅有 22 例(0.8%)患者发生新的淋巴结转移;5、10 和 15 年的淋巴结转移率分别为 0.9%、1.1%和 1.1%,非常低。
年轻的 PTMC 患者更有可能发生肿瘤生长。实现低正常范围的轻度 TSH 抑制可能会预防癌肿增大;然而,需要前瞻性研究得出更可靠的结论。