Nogueira Gabriel Martins, Silva Noel Lucas Oliveira Rodrigues, Moura Ana Flávia, Duarte Silveira Marcelo Augusto, Moura-Neto José A
Department of Medicine, Bahiana School of Medicine and Public Health, Salvador 40290-000, Bahia, Brazil.
Department of Nephrology, D'Or Institute for Research and Education, Hospital São Rafael, Salvador 41253900, Bahia, Brazil.
World J Virol. 2022 Sep 25;11(5):283-292. doi: 10.5501/wjv.v11.i5.283.
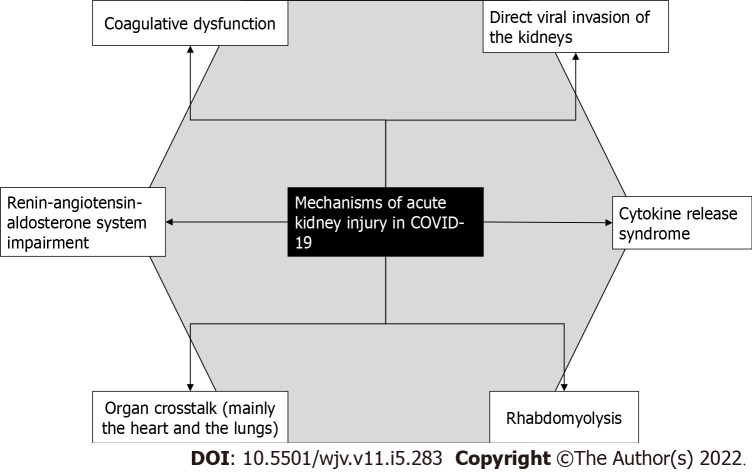
Acute kidney injury (AKI) and electrolyte disorders are important complications of hospitalized coronavirus disease 2019 (COVID-19) patients. AKI is thought to occur due to multiple pathophysiological mechanisms, such as multiple organ dysfunction (mainly cardiac and respiratory), direct viral entry in the renal tubules, and cytokine release syndrome. AKI is present in approximately one in every ten hospitalized COVID-19 patients. The incidence rates of AKI increase in patients who are admitted to the intensive care unit (ICU), with levels higher than 50%. Additionally, renal replacement therapy (RRT) is used in 7% of all AKI cases, but in nearly 20% of patients admitted to an ICU. COVID-19 patients with AKI are considered moderate-to-severe cases and are managed with multiple interdisciplinary conducts. AKI acts as a risk factor for mortality in severe acute respiratory syndrome coronavirus 2 infection, especially when RRT is needed. Electrolyte disorders are also common manifestations in hospitalized COVID-19 patients, mainly hyponatremia, hypokalemia, and hypocalcemia. Hyponatremia occurs due to a combination of syndrome of inappropriate secretion of antidiuretic hormone and gastrointestinal fluid loss from vomiting and diarrhea. When it comes to hypokalemia, its mechanism is not fully understood but may derive from hyperaldosteronism due to renin angiotensin aldosterone system overstimulation and gastrointestinal fluid loss as well. The clinical features of hypokalemia in COVID-19 are similar to those in other conditions. Hypocalcemia is the most common electrolyte disorder in COVID-19 and seems to occur because of vitamin D deficiency and parathyroid imbalance. It is also highly associated with longer hospital and ICU stay.
急性肾损伤(AKI)和电解质紊乱是2019冠状病毒病(COVID-19)住院患者的重要并发症。AKI被认为是由多种病理生理机制引起的,如多器官功能障碍(主要是心脏和呼吸功能)、病毒直接侵入肾小管以及细胞因子释放综合征。每十名住院的COVID-19患者中约有一人出现AKI。入住重症监护病房(ICU)的患者中AKI的发病率增加,超过50%。此外,在所有AKI病例中,7%的患者使用了肾脏替代治疗(RRT),但在入住ICU的患者中这一比例接近20%。患有AKI的COVID-19患者被视为中重度病例,需要多学科联合治疗。AKI是严重急性呼吸综合征冠状病毒2感染患者死亡的危险因素,尤其是在需要进行RRT时。电解质紊乱也是COVID-19住院患者的常见表现,主要是低钠血症、低钾血症和低钙血症。低钠血症是由于抗利尿激素分泌不当综合征以及呕吐和腹泻导致的胃肠道液体流失共同作用引起的。至于低钾血症,其机制尚未完全明确,但可能源于肾素-血管紧张素-醛固酮系统过度刺激导致的醛固酮增多症以及胃肠道液体流失。COVID-19患者低钾血症的临床特征与其他情况相似。低钙血症是COVID-19中最常见的电解质紊乱,似乎是由于维生素D缺乏和甲状旁腺失衡所致。它也与住院和ICU住院时间延长高度相关。