From the Department of Neuroinflammation (R.C., F.P.C., C.T., A.B., W.B., F.D.A., I.D.L.P., F.G., L.H., L.M., A.T., M.Y., A.T.T., Y.H.R.C.P.C.H., F.B., O.C.), Queen Square MS Centre, UCL Queen Square Institute of Neurology, Faculty of Brain Science, University College of London; Department of Medicine (R.C.), Surgery and Neuroscience, University of Siena, Italy; Department of Medical Physics and Biomedical Engineering (F.P.C., B.K., F.B.), Centre for Medical Imaging Computing, University College of London; Universitat Oberta de Catalunya (F.P.C.), Barcelona, Spain; MS Centre of Catalonia (Cemcat) (C.T.), Vall d'Hebron Institute of Research, Spain; Radiomics Group (F.G.), Vall d'Hebron Institute of Oncology, Vall d'Hebron Barcelona Barcelona, Spain; Department of Biomedical Imaging and Image Guided Therapy (L.H.), Medical University of Vienna, Austria; NMO Clinical Service at the Walton Centre (A.J.), Liverpool, United Kingdom; Division of Multiple Sclerosis and Autoimmune Neurology (A.J.), Neurological Institute, Cleveland Clinic Abu Dhabi, United Arab Emirates; Division of Brain Sciences (R.S.N.), Department of Medicine, Imperial College London; National Institute for Health Research (NIHR) (A.T., F.B., O.C.), University College London Hospitals (UCLH), Biomedical Research Centre; and Department of Radiology and Nuclear Medicine (F.B.), Amsterdam University Medical Centre, the Netherlands.
Neurology. 2023 Jan 17;100(3):e308-e323. doi: 10.1212/WNL.0000000000201465. Epub 2022 Oct 3.
Relapsing-remitting multiple sclerosis (RRMS), aquaporin-4 antibody-positive neuromyelitis optica spectrum disorder (AQP4-NMOSD), and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) may have overlapping clinical features. There is an unmet need for imaging markers that differentiate between them when serologic testing is unavailable or ambiguous. We assessed whether imaging characteristics typical of MS discriminate RRMS from AQP4-NMOSD and MOGAD, alone and in combination.
Adult, nonacute patients with RRMS, APQ4-NMOSD, and MOGAD and healthy controls were prospectively recruited at the National Hospital for Neurology and Neurosurgery (London, United Kingdom) and the Walton Centre (Liverpool, United Kingdom) between 2014 and 2019. They underwent conventional and advanced brain, cord, and optic nerve MRI and optical coherence tomography (OCT).
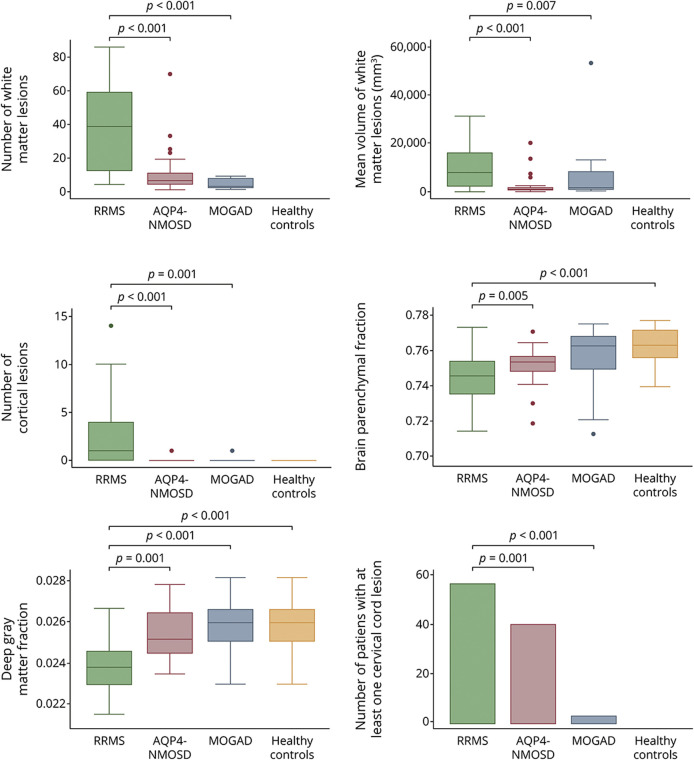
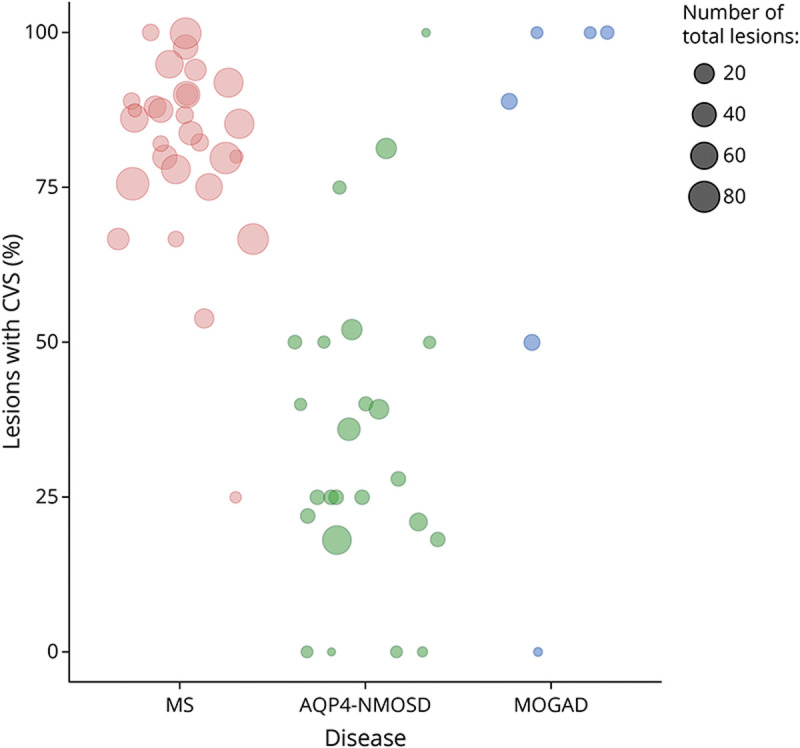
A total of 91 consecutive patients (31 RRMS, 30 APQ4-NMOSD, and 30 MOGAD) and 34 healthy controls were recruited. The most accurate measures differentiating RRMS from AQP4-NMOSD were the proportion of lesions with the central vein sign (CVS) (84% vs 33%, accuracy/specificity/sensitivity: 91/88/93%, < 0.001), followed by cortical lesions (median: 2 [range: 1-14] vs 1 [0-1], accuracy/specificity/sensitivity: 84/90/77%, = 0.002) and white matter lesions (mean: 39.07 [±25.8] vs 9.5 [±14], accuracy/specificity/sensitivity: 78/84/73%, = 0.001). The combination of higher proportion of CVS, cortical lesions, and optic nerve magnetization transfer ratio reached the highest accuracy in distinguishing RRMS from AQP4-NMOSD (accuracy/specificity/sensitivity: 95/92/97%, < 0.001). The most accurate measures favoring RRMS over MOGAD were white matter lesions (39.07 [±25.8] vs 1 [±2.3], accuracy/specificity/sensitivity: 94/94/93%, = 0.006), followed by cortical lesions (2 [1-14] vs 1 [0-1], accuracy/specificity/sensitivity: 84/97/71%, = 0.004), and retinal nerve fiber layer thickness (RNFL) (mean: 87.54 [±13.83] vs 75.54 [±20.33], accuracy/specificity/sensitivity: 80/79/81%, = 0.009). Higher cortical lesion number combined with higher RNFL thickness best differentiated RRMS from MOGAD (accuracy/specificity/sensitivity: 84/92/77%, < 0.001).
Cortical lesions, CVS, and optic nerve markers achieve a high accuracy in distinguishing RRMS from APQ4-NMOSD and MOGAD. This information may be useful in clinical practice, especially outside the acute phase and when serologic testing is ambiguous or not promptly available.
This study provides Class II evidence that selected conventional and advanced brain, cord, and optic nerve MRI and OCT markers distinguish adult patients with RRMS from AQP4-NMOSD and MOGAD.
复发缓解型多发性硬化症(RRMS)、水通道蛋白 4 抗体阳性视神经脊髓炎谱系疾病(AQP4-NMOSD)和髓鞘少突胶质细胞糖蛋白抗体相关性疾病(MOGAD)可能具有重叠的临床特征。在血清学检测不可用或不明确时,需要影像学标志物来区分它们,但目前这一需求尚未得到满足。我们评估了典型的 MS 影像学特征是否可以单独或组合区分 RRMS 与 AQP4-NMOSD 和 MOGAD。
2014 年至 2019 年,在英国国家神经学和神经外科学院(伦敦)和沃尔顿中心(利物浦)前瞻性招募了成人非急性 RRMS、AQP4-NMOSD 和 MOGAD 患者以及健康对照者。他们接受了常规和高级脑部、脊髓和视神经 MRI 及光学相干断层扫描(OCT)检查。
共纳入 91 例连续患者(31 例 RRMS、30 例 AQP4-NMOSD 和 30 例 MOGAD)和 34 例健康对照者。区分 RRMS 与 AQP4-NMOSD 最准确的指标是伴有中央静脉征(CVS)的病灶比例(84%比 33%,准确性/特异性/敏感性:91/88/93%,<0.001),其次是皮质病灶(中位数:2[范围:1-14]比 1[0-1],准确性/特异性/敏感性:84/90/77%,=0.002)和白质病灶(均值:39.07[±25.8]比 9.5[±14],准确性/特异性/敏感性:78/84/73%,=0.001)。CVS 比例较高、皮质病灶和视神经磁化传递比的组合在区分 RRMS 与 AQP4-NMOSD 方面达到了最高的准确性(准确性/特异性/敏感性:95/92/97%,<0.001)。有利于 RRMS 的最准确指标是白质病灶(39.07[±25.8]比 1[±2.3],准确性/特异性/敏感性:94/94/93%,=0.006),其次是皮质病灶(2[1-14]比 1[0-1],准确性/特异性/敏感性:84/97/71%,=0.004)和视网膜神经纤维层厚度(RNFL)(均值:87.54[±13.83]比 75.54[±20.33],准确性/特异性/敏感性:80/79/81%,=0.009)。皮质病灶数量较高与 RNFL 厚度较高相结合可最佳地区分 RRMS 与 MOGAD(准确性/特异性/敏感性:84/92/77%,<0.001)。
皮质病灶、CVS 和视神经标志物在区分 RRMS 与 AQP4-NMOSD 和 MOGAD 方面具有很高的准确性。这些信息在临床实践中可能有用,尤其是在急性期之外,当血清学检测不明确或不能及时获得时。
本研究提供了 II 级证据,表明选定的常规和高级脑、脊髓和视神经 MRI 和 OCT 标志物可区分成人 RRMS 患者与 AQP4-NMOSD 和 MOGAD。