Filippatou Angeliki G, Mukharesh Loulwah, Saidha Shiv, Calabresi Peter A, Sotirchos Elias S
Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Front Neurol. 2020 Oct 8;11:540156. doi: 10.3389/fneur.2020.540156. eCollection 2020.
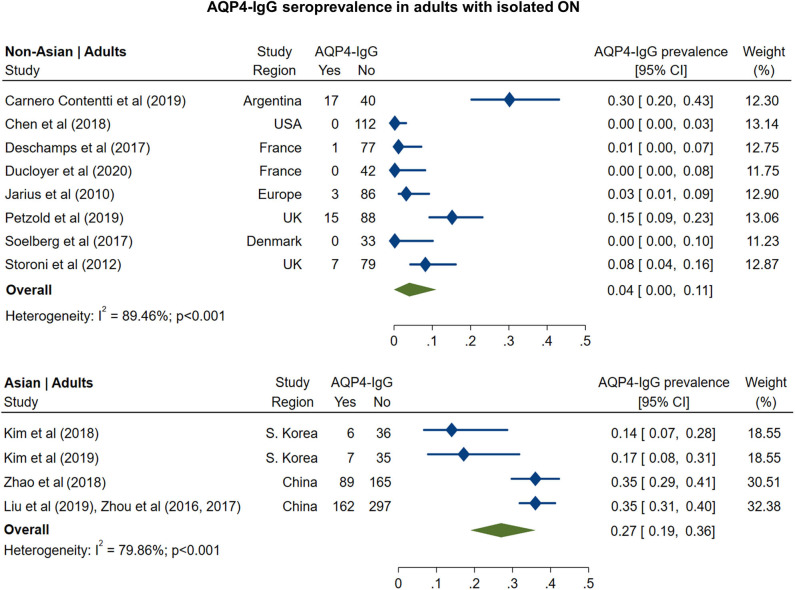
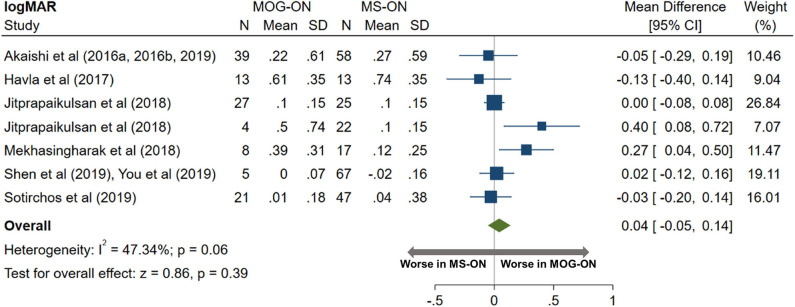
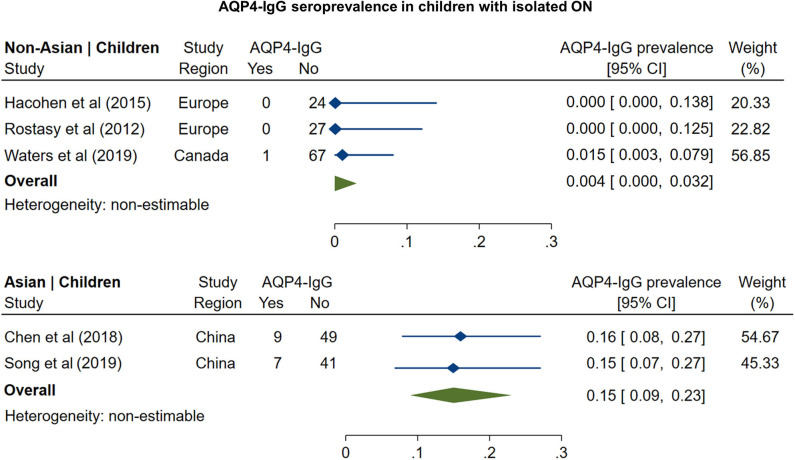
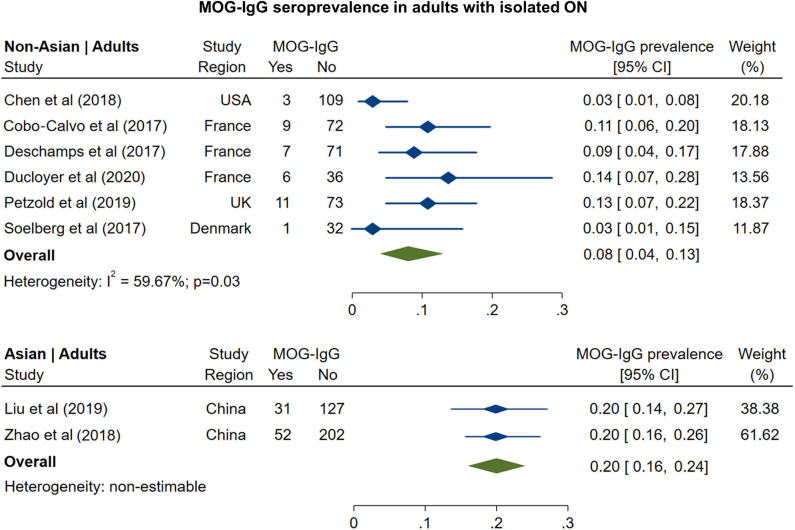
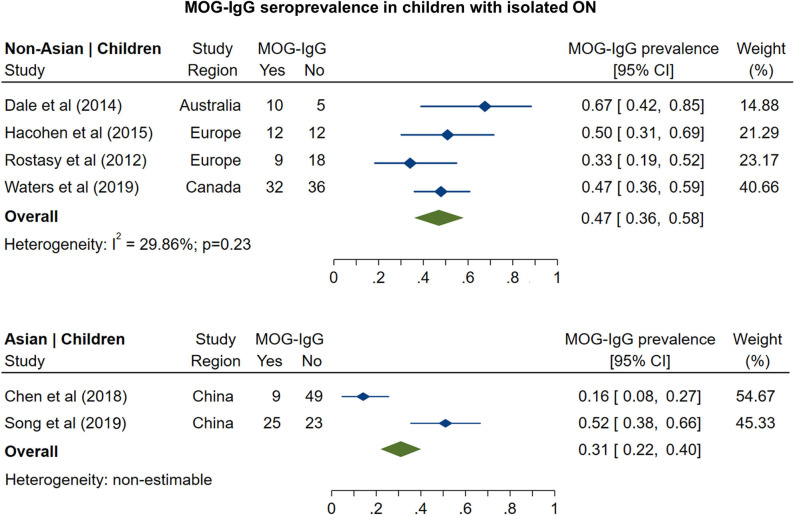
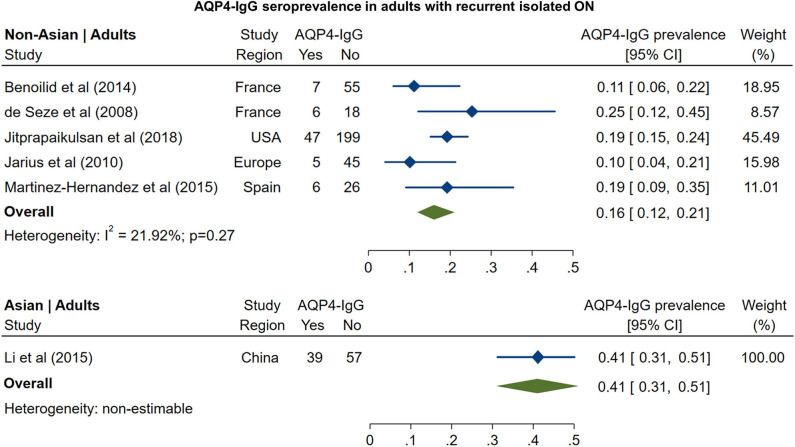
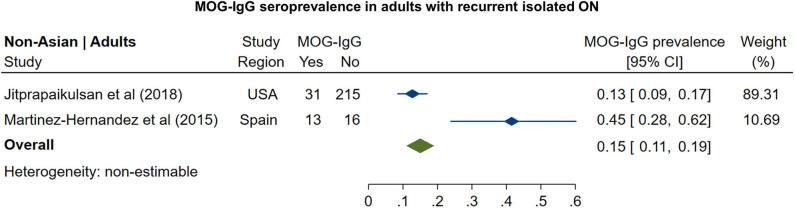
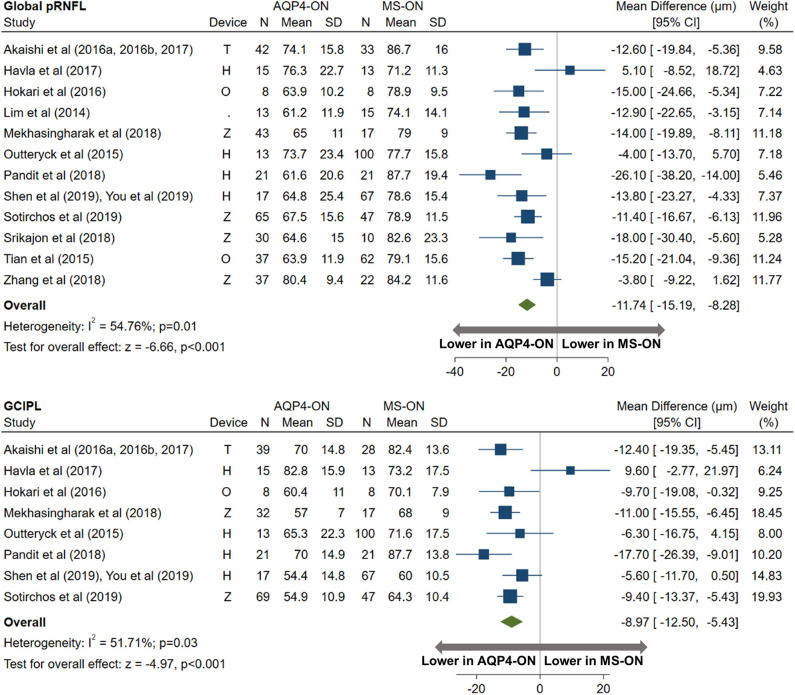
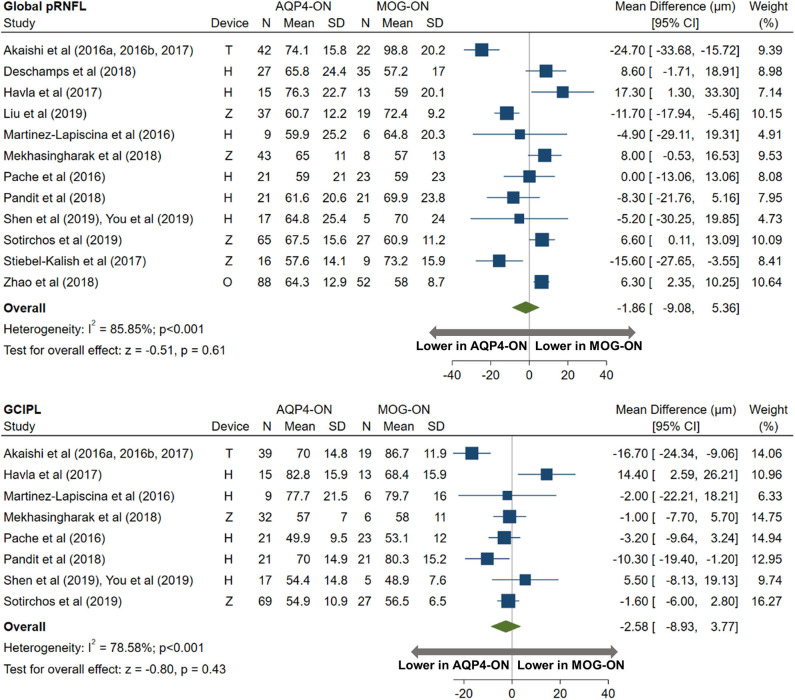
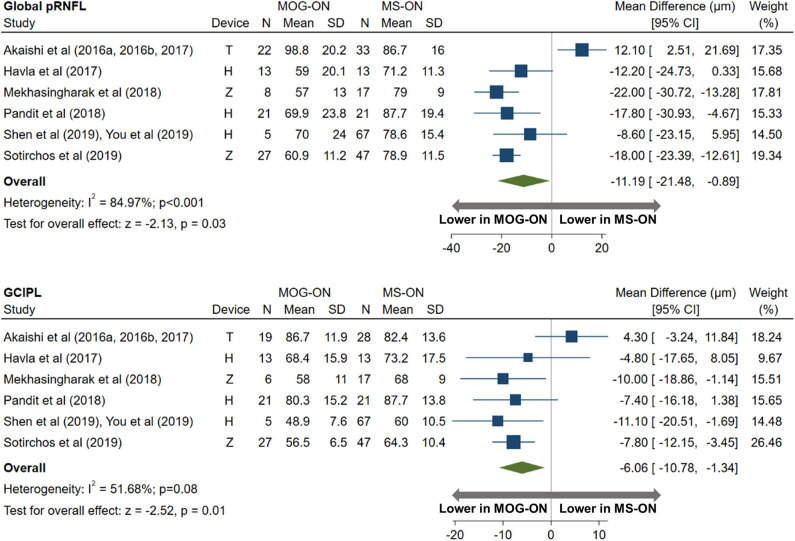
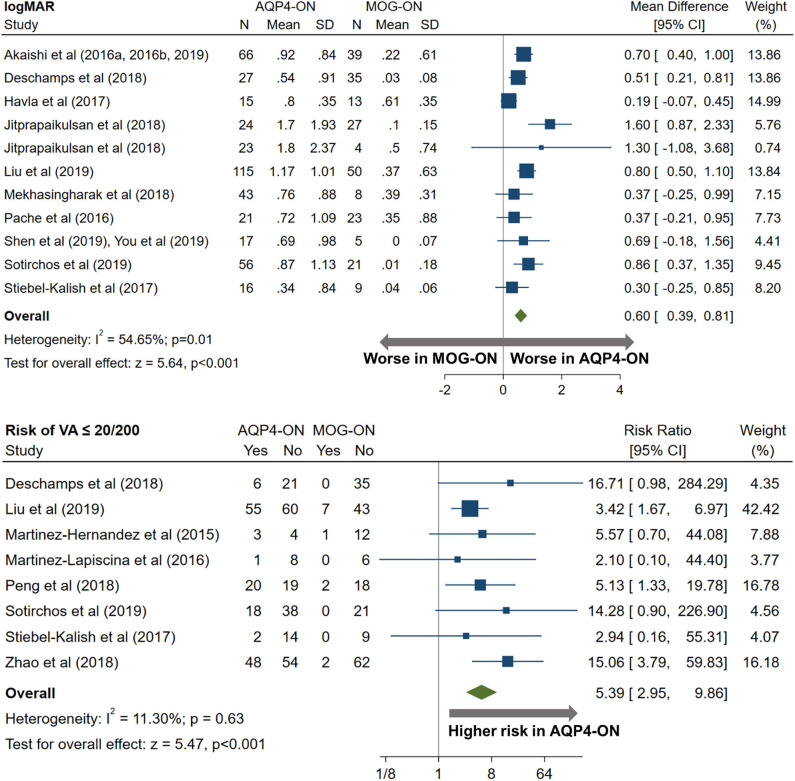
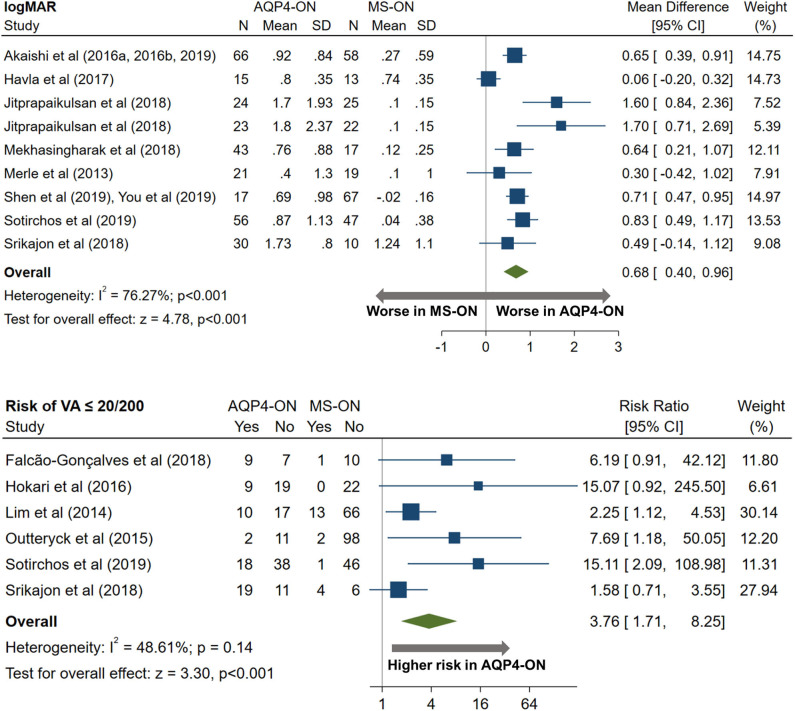
Optic neuritis (ON) is a cardinal manifestation of multiple sclerosis (MS), aquaporin-4 (AQP4)-IgG-, and myelin oligodendrocyte glycoprotein (MOG)-IgG-associated disease. However, the prevalence of AQP4-IgG seropositivity and MOG-IgG seropositivity in isolated ON is unclear, and studies comparing visual outcomes and optical coherence tomography (OCT)-derived structural retinal measures between MS-ON, AQP4-ON, and MOG-ON eyes are limited by small sample sizes. (1) To assess the prevalence of AQP4-IgG and MOG-IgG seropositivity among patients presenting with isolated ON; (2) to compare visual outcomes and OCT measures between AQP4-ON, MOG-ON, and MS-ON eyes. In this systematic review and meta-analysis, a total of 65 eligible studies were identified by PubMed search. Statistical analyses were performed with random effects models. In adults with isolated ON, AQP4-IgG seroprevalence was 4% in non-Asian and 27% in Asian populations, whereas MOG-IgG seroprevalence was 8 and 20%, respectively. In children, AQP4-IgG seroprevalence was 0.4% in non-Asian and 15% in Asian populations, whereas MOG-IgG seroprevalence was 47 and 31%, respectively. AQP4-ON eyes had lower peri-papillary retinal nerve fiber layer (pRNFL; -11.7 μm, 95% CI: -15.2 to -8.3 μm) and macular ganglion cell + inner plexiform layer (GCIPL; -9.0 μm, 95% CI: -12.5 to -5.4 μm) thicknesses compared with MS-ON eyes. Similarly, pRNFL (-11.2 μm, 95% CI: -21.5 to -0.9 μm) and GCIPL (-6.1 μm, 95% CI: -10.8 to -1.3 μm) thicknesses were lower in MOG-ON compared to MS-ON eyes, but did not differ between AQP4-ON and MOG-ON eyes (pRNFL: -1.9 μm, 95% CI: -9.1 to 5.4 μm; GCIPL: -2.6 μm, 95% CI: -8.9 to 3.8 μm). Visual outcomes were worse in AQP4-ON compared to both MOG-ON (mean logMAR difference: 0.60, 95% CI: 0.39 to 0.81) and MS-ON eyes (mean logMAR difference: 0.68, 95% CI: 0.40 to 0.96) but were similar in MOG-ON and MS-ON eyes (mean logMAR difference: 0.04, 95% CI: -0.05 to 0.14). AQP4-IgG- and MOG-IgG-associated disease are important diagnostic considerations in adults presenting with isolated ON, especially in Asian populations. Furthermore, MOG-IgG seroprevalence is especially high in pediatric isolated ON, in both non-Asian and Asian populations. Despite a similar severity of GCIPL and pRNFL thinning in AQP4-ON and MOG-ON, AQP4-ON is associated with markedly worse visual outcomes.
视神经炎(ON)是多发性硬化(MS)、水通道蛋白4(AQP4)-IgG相关性疾病和髓鞘少突胶质细胞糖蛋白(MOG)-IgG相关性疾病的主要表现。然而,孤立性ON中AQP4-IgG血清阳性率和MOG-IgG血清阳性率尚不清楚,且比较MS-ON、AQP4-ON和MOG-ON患者视力结果及光学相干断层扫描(OCT)得出的视网膜结构测量值的研究因样本量小而受到限制。(1)评估孤立性ON患者中AQP4-IgG和MOG-IgG血清阳性率;(2)比较AQP4-ON、MOG-ON和MS-ON患者的视力结果及OCT测量值。在这项系统评价和荟萃分析中,通过PubMed检索共确定了65项符合条件的研究。采用随机效应模型进行统计分析。在孤立性ON的成人患者中,非亚洲人群的AQP4-IgG血清阳性率为4%,亚洲人群为27%,而MOG-IgG血清阳性率分别为8%和20%。在儿童中,非亚洲人群的AQP4-IgG血清阳性率为0.4%,亚洲人群为15%,而MOG-IgG血清阳性率分别为47%和31%。与MS-ON患者相比,AQP4-ON患者的视乳头周围视网膜神经纤维层(pRNFL;-11.7μm,95%CI:-15.2至-8.3μm)和黄斑神经节细胞+内丛状层(GCIPL;-9.0μm,95%CI:-12.5至-5.4μm)厚度更低。同样,与MS-ON患者相比,MOG-ON患者的pRNFL(-11.2μm,95%CI:-21.5至-0.9μm)和GCIPL(-6.1μm,95%CI:-10.8至-1.3μm)厚度更低,但AQP4-ON和MOG-ON患者之间无差异(pRNFL:-1.9μm,95%CI:-9.1至5.4μm;GCIPL:-2.6μm,95%CI:-8.9至3.8μm)。与MOG-ON(平均logMAR差值:0.60,95%CI:0.39至0.81)和MS-ON患者(平均logMAR差值:0.68,95%CI:0.40至0.96)相比,AQP4-ON患者的视力结果更差,但MOG-ON和MS-ON患者的视力结果相似(平均logMAR差值:0.04,95%CI:-0.05至0.14)。AQP4-IgG和MOG-IgG相关性疾病是孤立性ON成人患者重要的诊断考虑因素,尤其是在亚洲人群中。此外,在非亚洲和亚洲人群的儿童孤立性ON中,MOG-IgG血清阳性率特别高。尽管AQP4-ON和MOG-ON患者的GCIPL和pRNFL变薄程度相似,但AQP4-ON与明显更差的视力结果相关。