Nuffield Department of Primary Care Health Sciences, Medical Sciences Division, University of Oxford, Oxford, United Kingdom.
Representing the Nordic Countries Childhood Survival Group, Department of Cancer Epidemiology, Lund University, Lund, Sweden.
JAMA Oncol. 2022 Dec 1;8(12):1756-1764. doi: 10.1001/jamaoncol.2022.4425.
Meningioma is the most common subsequent neoplasm following cranial irradiation among survivors of childhood cancer, but there are still uncertainties regarding the magnitude of the radiation dose-response association, potential modifiers of radiation risks, and the role of chemotherapy.
To evaluate meningioma risk in survivors of childhood cancer following radiotherapy and chemotherapy and identify possible modifying factors of radiation-associated risk.
DESIGN, SETTING, AND PARTICIPANTS: This international case-control study pooled data from 4 nested case-control studies of survivors of childhood cancer diagnosed between 1942 and 2000, followed through 2016. Cases were defined as participants diagnosed with a subsequent meningioma. Controls were matched to cases based on sex, age at first cancer diagnosis, and duration of follow-up. Data were analyzed from July 2019 to June 2022.
Radiation dose (Gy) to the meningioma site and cumulative chemotherapy doses, including intrathecal and systemic methotrexate doses.
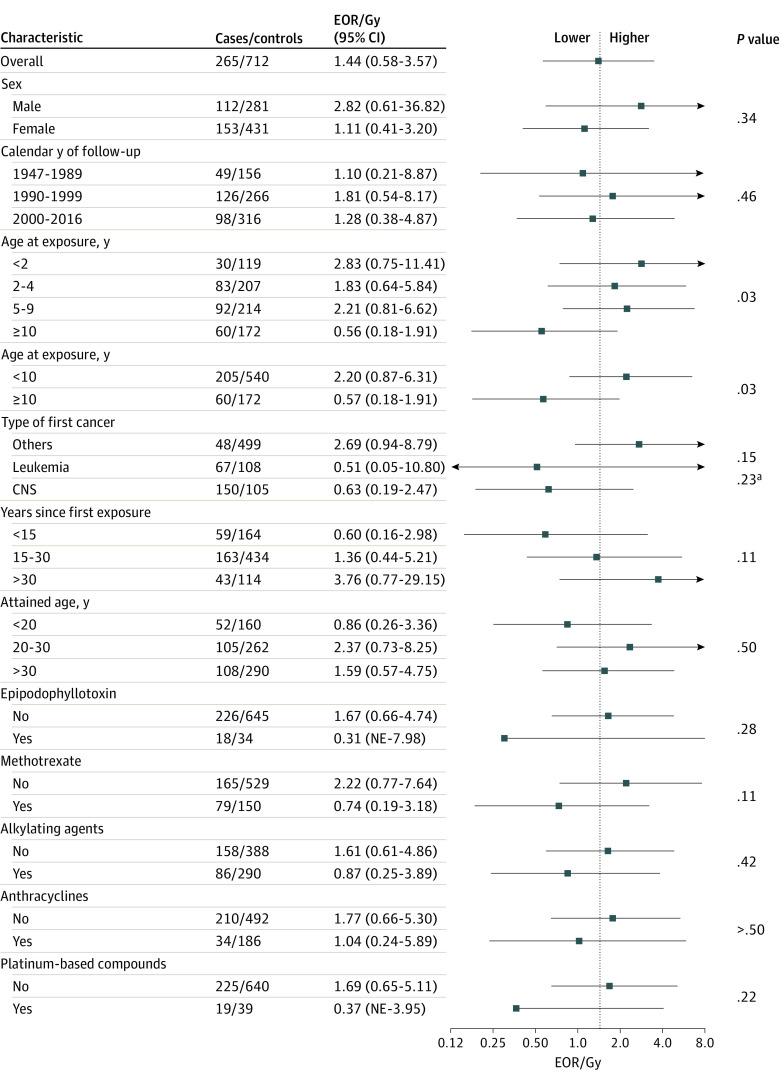
The main outcome was subsequent meningioma, assessed using odds ratios (ORs) and excess odds ratios per gray (EOR/Gy).
The analysis included 273 survivors of childhood cancer who developed meningioma (cases) and 738 survivors who did not (controls), with a total of 1011 individuals (median [IQR] age at first cancer diagnosis 5.0 [3.0-9.2] years; 599 [59.2%] female). Median (IQR) time since first cancer was 21.5 (15.0-27.0) years. Increasing radiation dose was associated with increased risk of meningioma (EOR/Gy, 1.44; 95% CI, 0.62-3.61), and there was no evidence of departure from linearity (P = .90). Compared with survivors who were not exposed to radiation therapy, those who received doses of 24 Gy or more had more than 30-fold higher odds of meningioma (OR, 33.66; 95% CI, 14.10-80.31). The radiation dose-response association was significantly lower among patients treated at age 10 years or older compared with those treated before age 10 years (EOR/Gy, 0.57; 95% CI, 0.18-1.91 vs 2.20; 95% CI, 0.87-6.31; P for heterogeneity = .03). Risk associated with radiation remained significantly elevated 30 years after exposure (EOR/Gy, 3.76; 95% CI, 0.77-29.15). We found an increased risk of meningioma among children who had received methotrexate (OR, 3.43; 95% CI, 1.56-7.57), but no evidence of a dose-response association or interaction with radiation dose.
These findings suggest that the meninges are highly radiosensitive, especially for children treated before age 10 years. These results support the reduction in whole-brain irradiation over recent decades and the prioritization of approaches that limit radiation exposure in healthy tissue for children. The persistence of elevated risks of meningiomas for 30 years after cranial radiotherapy could help inform surveillance guidelines.
脑膜瘤是儿童癌症幸存者接受颅部放射治疗后最常见的继发肿瘤,但对于放射剂量反应关联的幅度、潜在的放射风险修饰因子以及化疗的作用仍存在不确定性。
评估儿童癌症幸存者在接受放射治疗和化疗后发生脑膜瘤的风险,并确定与放射相关风险的可能修饰因子。
设计、设置和参与者:这项国际病例对照研究汇集了 4 项嵌套病例对照研究的数据,这些研究纳入了 1942 年至 2000 年间诊断的儿童癌症幸存者,并随访至 2016 年。病例定义为诊断为后续脑膜瘤的参与者。对照病例按照性别、首次癌症诊断时的年龄和随访时间与病例相匹配。数据于 2019 年 7 月至 2022 年 6 月进行分析。
脑膜瘤部位的放射剂量(Gy)和累积化疗剂量,包括鞘内和全身甲氨蝶呤剂量。
主要结果是后续脑膜瘤,使用比值比(OR)和每戈瑞的超额比值(EOR/Gy)进行评估。
该分析纳入了 273 名患有脑膜瘤的儿童癌症幸存者(病例)和 738 名未患有脑膜瘤的幸存者(对照),共计 1011 人(首次癌症诊断的中位年龄[IQR]为 5.0[3.0-9.2]岁;599[59.2%]为女性)。中位数(IQR)自首次癌症以来的时间为 21.5(15.0-27.0)年。放射剂量的增加与脑膜瘤风险的增加相关(EOR/Gy,1.44;95%CI,0.62-3.61),且不存在线性偏离的证据(P=0.90)。与未接受放射治疗的幸存者相比,接受 24 Gy 或更高剂量放射治疗的幸存者患脑膜瘤的几率高出 30 多倍(OR,33.66;95%CI,14.10-80.31)。与 10 岁以下接受治疗的患者相比,10 岁及以上接受治疗的患者的放射剂量-反应关系显著较低(EOR/Gy,0.57;95%CI,0.18-1.91 比 2.20;95%CI,0.87-6.31;P 值用于异质性=0.03)。暴露后 30 年,与放射相关的风险仍然显著升高(EOR/Gy,3.76;95%CI,0.77-29.15)。我们发现接受甲氨蝶呤治疗的儿童脑膜瘤风险增加(OR,3.43;95%CI,1.56-7.57),但没有发现剂量-反应关系或与放射剂量的相互作用。
这些发现表明脑膜对放射非常敏感,尤其是对于 10 岁以下接受治疗的儿童。这些结果支持了近几十年来全脑照射减少的做法,并优先考虑在健康组织中限制放射暴露的方法,以保护儿童。在颅部放射治疗后 30 年内,脑膜瘤风险持续升高,这可能有助于制定监测指南。