Department of Medicine, Division of Cardiology, Johns Hopkins Hospital, Baltimore, MD (A.G., R.T.C., C. Tichnell, B.M., H.T., H.C., C.A.J.).
Department of Cardiology, University Heart Center Zurich, University Hospital Zurich' Switzerland (S.C., C.B.B., F.D., A.M.S.).
Circulation. 2022 Nov 8;146(19):1434-1443. doi: 10.1161/CIRCULATIONAHA.122.060866. Epub 2022 Oct 7.
A novel risk calculator based on clinical characteristics and noninvasive tests that predicts the onset of clinical sustained ventricular arrhythmias (VA) in patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) has been proposed and validated by recent studies. It remains unknown whether programmed ventricular stimulation (PVS) provides additional prognostic value.
All patients with a definite ARVC diagnosis, no history of sustained VAs at diagnosis, and PVS performed at baseline were extracted from 6 international ARVC registries. The calculator-predicted risk for sustained VA (sustained or implantable cardioverter defibrillator treated ventricular tachycardia [VT] or fibrillation, [aborted] sudden cardiac arrest) was assessed in all patients. Independent and combined performance of the risk calculator and PVS on sustained VA were assessed during a 5-year follow-up period.
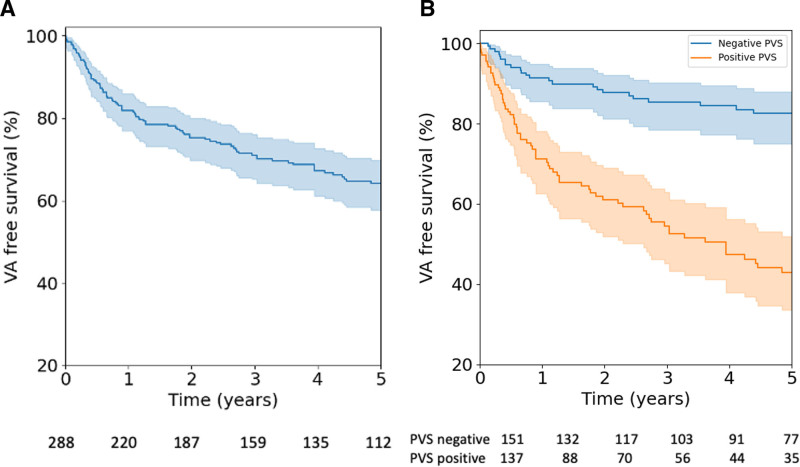
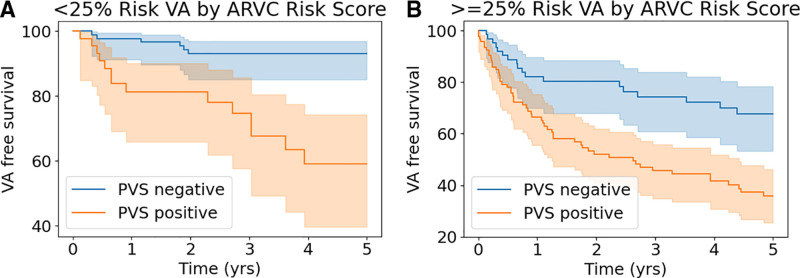
Two hundred eighty-eight patients (41.0±14.5 years, 55.9% male, right ventricular ejection fraction 42.5±11.1%) were enrolled. At PVS, 137 (47.6%) patients had inducible ventricular tachycardia. During a median of 5.31 [2.89-10.17] years of follow-up, 83 (60.6%) patients with a positive PVS and 37 (24.5%) with a negative PVS experienced sustained VA (<0.001). Inducible ventricular tachycardia predicted clinical sustained VA during the 5-year follow-up and remained an independent predictor after accounting for the calculator-predicted risk (HR, 2.52 [1.58-4.02]; <0.001). Compared with ARVC risk calculator predictions in isolation (C-statistic 0.72), addition of PVS inducibility showed improved prediction of VA events (C-statistic 0.75; log-likelihood ratio for nested models, <0.001). PVS inducibility had a 76% [67-84] sensitivity and 68% [61-74] specificity, corresponding to log-likelihood ratios of 2.3 and 0.36 for inducible (likelihood ratio+) and noninducible (likelihood ratio-) patients, respectively. In patients with a ARVC risk calculator-predicted risk of clinical VA events <25% during 5 years (ie, low/intermediate subgroup), PVS had a 92.6% negative predictive value.
PVS significantly improved risk stratification above and beyond the calculator-predicted risk of VA in a primary prevention cohort of patients with ARVC, mainly for patients considered to be at low and intermediate risk by the clinical risk calculator.
最近的研究提出并验证了一种基于临床特征和无创检查的新型风险计算器,可预测致心律失常性右心室心肌病(ARVC)患者临床持续性室性心律失常(VA)的发生。目前尚不清楚程控心室刺激(PVS)是否提供了额外的预后价值。
从 6 个国际 ARVC 注册中心提取所有明确 ARVC 诊断、诊断时无持续性 VA 病史且基线时进行 PVS 的患者。在所有患者中评估计算器预测的持续性 VA(持续性或植入式心脏复律除颤器治疗的室性心动过速[VT]或颤动,[已终止]心源性猝死)风险。在 5 年随访期间,评估风险计算器和 PVS 对持续性 VA 的独立和联合性能。
共纳入 288 例患者(41.0±14.5 岁,55.9%为男性,右心室射血分数 42.5±11.1%)。在 PVS 中,137 例(47.6%)患者诱发性室性心动过速。在中位 5.31[2.89-10.17]年的随访期间,83 例(60.6%)PVS 阳性和 37 例(24.5%)PVS 阴性的患者发生持续性 VA(<0.001)。在 5 年随访期间,诱发性室性心动过速可预测临床持续性 VA,且在考虑计算器预测风险后仍为独立预测因素(HR,2.52[1.58-4.02];<0.001)。与 ARVC 风险计算器预测值(C 统计量 0.72)相比,PVS 诱发性可改善 VA 事件的预测(C 统计量 0.75;嵌套模型的对数似然比,<0.001)。PVS 诱发性的敏感性为 76%[67-84],特异性为 68%[61-74],相应的对数似然比分别为 2.3 和 0.36,用于诱发性(似然比+)和非诱发性(似然比-)患者。在 ARVC 风险计算器预测的 5 年内临床 VA 事件风险<25%的患者(即低/中风险亚组)中,PVS 的阴性预测值为 92.6%。
在 ARVC 患者的一级预防队列中,PVS 显著提高了风险分层,且优于计算器预测的 VA 风险,主要用于临床风险计算器预测为低风险和中风险的患者。