Akiyama Goh, Ono Shimpei, Sekine Tetsuro, Usami Satoshi, Ogawa Rei
Department of Plastic, Reconstructive and Aesthetic Surgery, Nippon Medical School Hospital, 1-1-5 Sendagi Bunkyo-ku, Tokyo, 113-8603, Japan.
Department of Radiology, Nippon Medical School Musashi Kosugi Hospital, Kanagawa, Japan.
Dermatol Ther (Heidelb). 2022 Nov;12(11):2575-2587. doi: 10.1007/s13555-022-00820-z. Epub 2022 Oct 7.
Most lipomas are readily dissected and removed. However, some cases can pose surgical difficulties. This retrospective study sought to identify clinical and radiological risk factors that predict difficult lipoma resection and can be used in a clinically useful scoring system that predicts difficulty preoperatively.
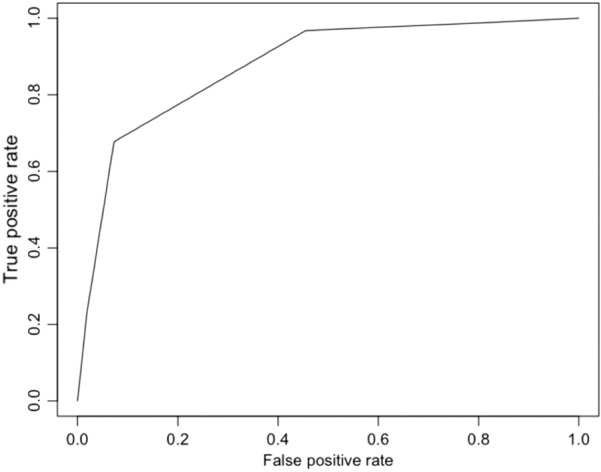
The study cohort consisted of all consecutive patients who underwent resection of pathology-confirmed lipoma during 2016-2018 at a tertiary care referral center in Tokyo, Japan. Surgical difficulty was defined as difficulty separating some/all of the tumor from the surrounding tissue by hand and inability to extract the tumor in one piece. Descriptive, univariate, and multivariate logistic regression analyses were conducted to identify predictive factors. The predictive accuracy of the scoring system that included these factors was assessed by tenfold cross-validation analysis. Receiver-operating curve (ROC) analysis was conducted to identify the optimal cutoff score for predicting surgical difficulty.
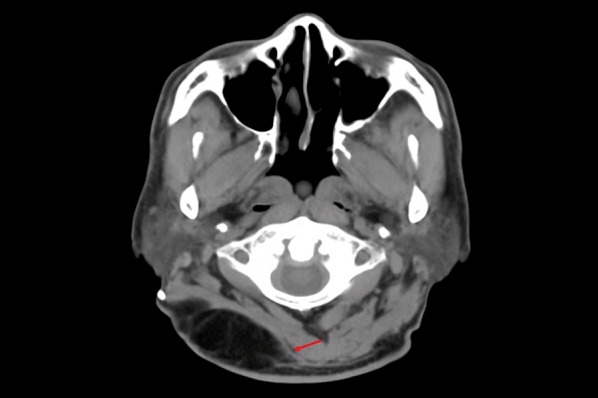
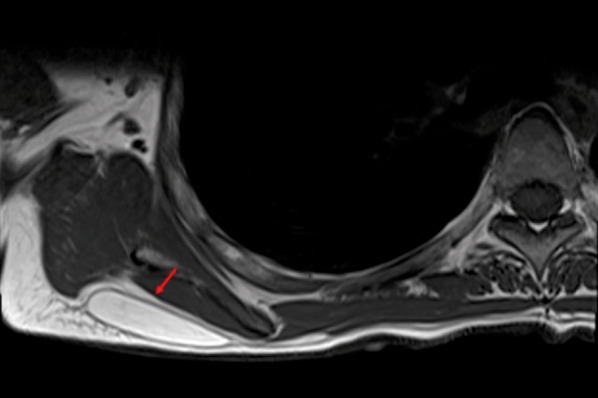
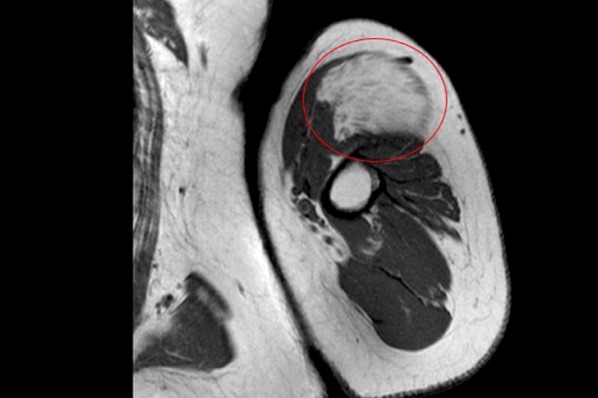
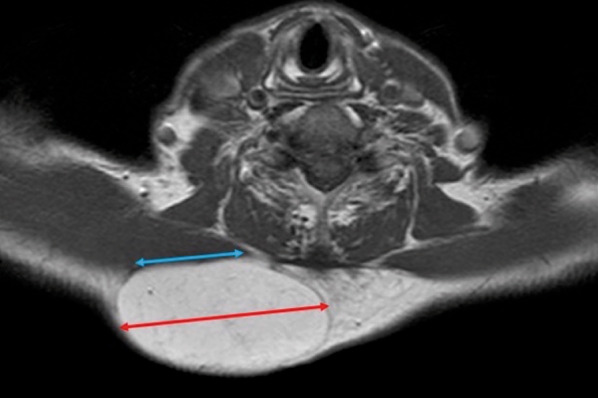
Of the 86 cases, 36% involved surgical difficulty. Multivariate analysis showed that subfascial intramuscular location (odds ratio 42.7, 95% confidence interval 3.0-608.0), broad touching of underlying structures (46.5, 3.7-586.0), in-flowing blood vessels (9.3, 1.1-78.5), and unclear boundaries (109.0, 1.1-1110.0) significantly predicted surgical difficulty. These factors were used to construct a 0-4 point scoring system (with one point per variable). On cross-validation, the accuracy of the scoring system was 82.4% (Cohen's kappa of 0.57). ROC analysis showed that scores ≥ 2 predicted surgical difficulty with sensitivity and specificity of 55% and 98%, respectively.
Our scoring system accurately predicted lipoma resection difficulty and may help operators prepare, thereby facilitating surgery.
大多数脂肪瘤易于解剖切除。然而,有些病例可能会带来手术困难。本回顾性研究旨在确定预测脂肪瘤切除困难的临床和放射学危险因素,并将其用于术前预测困难程度的临床实用评分系统。
研究队列包括2016年至2018年期间在日本东京一家三级医疗转诊中心接受病理确诊脂肪瘤切除术的所有连续患者。手术困难定义为手动将部分/全部肿瘤与周围组织分离困难以及无法完整取出肿瘤。进行描述性、单变量和多变量逻辑回归分析以确定预测因素。通过十折交叉验证分析评估包含这些因素的评分系统的预测准确性。进行受试者操作特征曲线(ROC)分析以确定预测手术困难的最佳截断分数。
86例病例中,36%存在手术困难。多变量分析显示,筋膜下肌内位置(比值比42.7,95%置信区间3.0 - 608.0)、与深层结构广泛接触(46.5,3.7 - 586.0)、有流入血管(9.3,1.1 - 78.5)以及边界不清(109.0,1.1 - 1110.0)显著预测手术困难。这些因素用于构建一个0 - 4分的评分系统(每个变量1分)。交叉验证时,评分系统的准确率为82.4%(科恩kappa系数为0.57)。ROC分析显示,评分≥2分预测手术困难的敏感性和特异性分别为55%和98%。
我们的评分系统准确预测了脂肪瘤切除困难,可能有助于手术医生做好准备,从而促进手术进行。