Ko Kyu-Yong, Jang Ji-Hun, Choi Seong-Huan, Baek Yong-Soo, Kwon Sung Woo, Park Sang-Don, Woo Seong-Ill, Kim Dae-Hyeok, Shin Sung-Hee
Division of Cardiology, Department of Internal Medicine, Inha University College of Medicine, Incheon, South Korea.
Front Cardiovasc Med. 2022 Sep 23;9:989012. doi: 10.3389/fcvm.2022.989012. eCollection 2022.
Left atrial (LA) remodeling is associated with adverse cardiovascular events, including heart failure (HF) and stroke in patients with atrial fibrillation (AF). However, there are limited data on the value of right atrial (RA) remodeling in this population. We investigated the prognostic role of RA enlargement in patients with non-valvular AF.
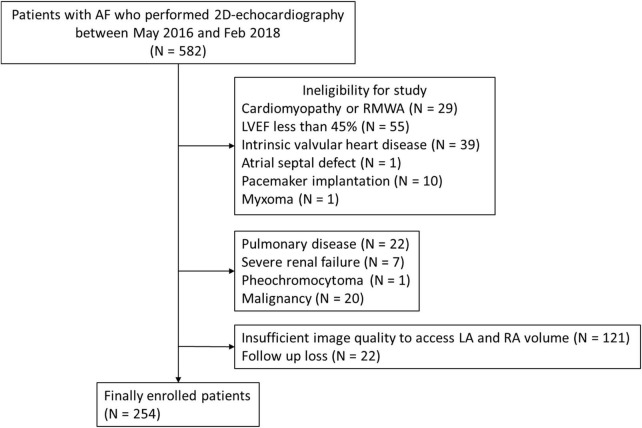
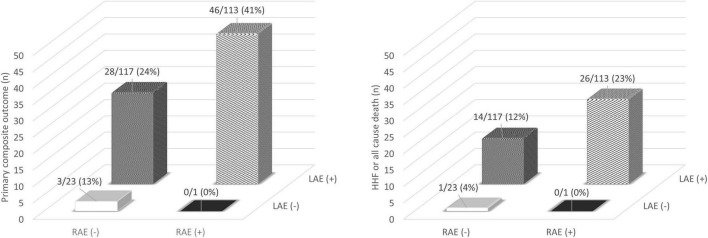
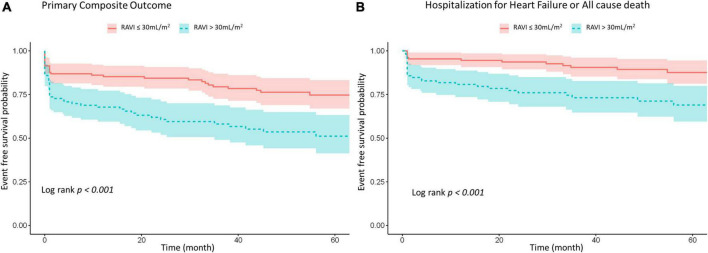
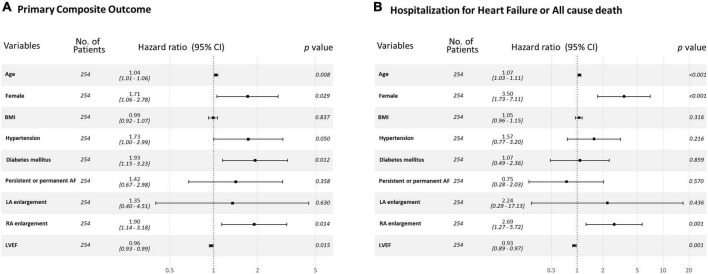
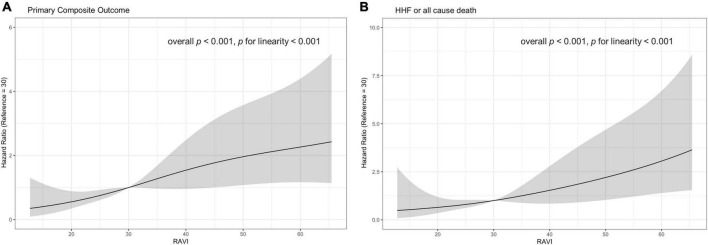
We analyzed 254 consecutive patients (age = 69 ± 12years, male:female = 165:89, mean left ventricular ejection fraction = 58.0 ± 7.2%) with non-valvular AF who underwent two-dimensional echocardiography from a single center. RA and LA volumes were measured from apical views and indexed to the body surface areas (right atrial volume index [RAVI] and left atrial volume index [LAVI]) and RAVI > 30mL/m and LAVI > 34mL/m were considered as enlarged. The relationship between RA enlargement and composite clinical outcome of hospitalization for HF (HHF), stroke, systemic embolism, or death from any cause was assessed. Right atrial (RA) enlargement was associated with older age and more frequent prevalence of persistent or permanent AF. During a median follow-up of 47.1 months, 77 patients (30%) had experienced primary composite outcome. In a multivariable model, RA enlargement, but not LA enlargement, was independently associated with adverse clinical outcomes even after adjusting for clinical and echocardiographic factors {adjusted hazard ratio [HR], 1.90 [95% confidence interval (CI), 1.14-3.18], = 0.014 for primary composite outcome; adjusted HR, 2.70 [95% CI, 1.27-5.67], = 0.001 for HHF or all cause death}.
RA enlargement was independently associated with an increased risk of HF, stroke, systemic embolization or death in patients with non-valvular AF, suggesting that RA volume can be helpful in assessing future cardiovascular risk in this population.
左心房(LA)重塑与不良心血管事件相关,包括心房颤动(AF)患者的心力衰竭(HF)和中风。然而,关于该人群右心房(RA)重塑价值的数据有限。我们研究了RA扩大在非瓣膜性AF患者中的预后作用。
我们分析了来自单一中心的254例连续的非瓣膜性AF患者(年龄=69±12岁,男性:女性=165:89,平均左心室射血分数=58.0±7.2%),这些患者接受了二维超声心动图检查。从心尖视图测量RA和LA容积,并根据体表面积进行指数化(右心房容积指数[RAVI]和左心房容积指数[LAVI]),RAVI>30mL/m²和LAVI>34mL/m²被认为是扩大。评估RA扩大与HF住院(HHF)、中风、系统性栓塞或任何原因死亡的综合临床结局之间的关系。右心房(RA)扩大与年龄较大以及持续性或永久性AF的更频繁患病率相关。在中位随访47.1个月期间,77例患者(30%)经历了主要综合结局。在多变量模型中,即使在调整临床和超声心动图因素后,RA扩大而非LA扩大与不良临床结局独立相关{主要综合结局的调整风险比[HR],1.90[95%置信区间(CI),1.14 - 3.18],P = 0.014;HHF或全因死亡的调整HR,2.70[95%CI,1.27 - 5.67],P = 0.001}。
RA扩大与非瓣膜性AF患者发生HF、中风、系统性栓塞或死亡的风险增加独立相关,提示RA容积有助于评估该人群未来的心血管风险。