Kaseb Ahmed O, Guan Yinghui, Gok Yavuz Betul, Abbas Alexander R, Lu Shan, Hasanov Elshad, Toh Han Chong, Verret Wendy, Wang Yulei
Department of Gastrointestinal Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Oncology Biomarker Development, Genentech Inc, South San Francisco, CA, USA.
J Hepatocell Carcinoma. 2022 Oct 11;9:1065-1079. doi: 10.2147/JHC.S369951. eCollection 2022.
Child-Turcotte-Pugh class A (CTP-A) in unresectable hepatocellular carcinoma (HCC) is the standard criterion for active therapy and clinical trial enrollment. We hypothesized that insulin-like growth factor-1 (IGF-1) derived scores may provide improved survival prediction over CTP classification. This study aimed to evaluate the potential prognostic and predictive effects of IGF-1 derived scores in the phase III IMbrave150 study.
Baseline and on-treatment serum IGF-1 levels from 371 patients were subjected to central analysis. Patients' IGF-1 score (1/2/3) and IGF-CTP score (A/B/C) were determined based on pre-specified cutoffs. Outcomes were analyzed by baseline and by on-treatment changes of the IGF-1 and IGF-CTP scores within and between the two treatment arms. The interaction between these scores and outcomes was assessed using univariate and multivariate analyses.
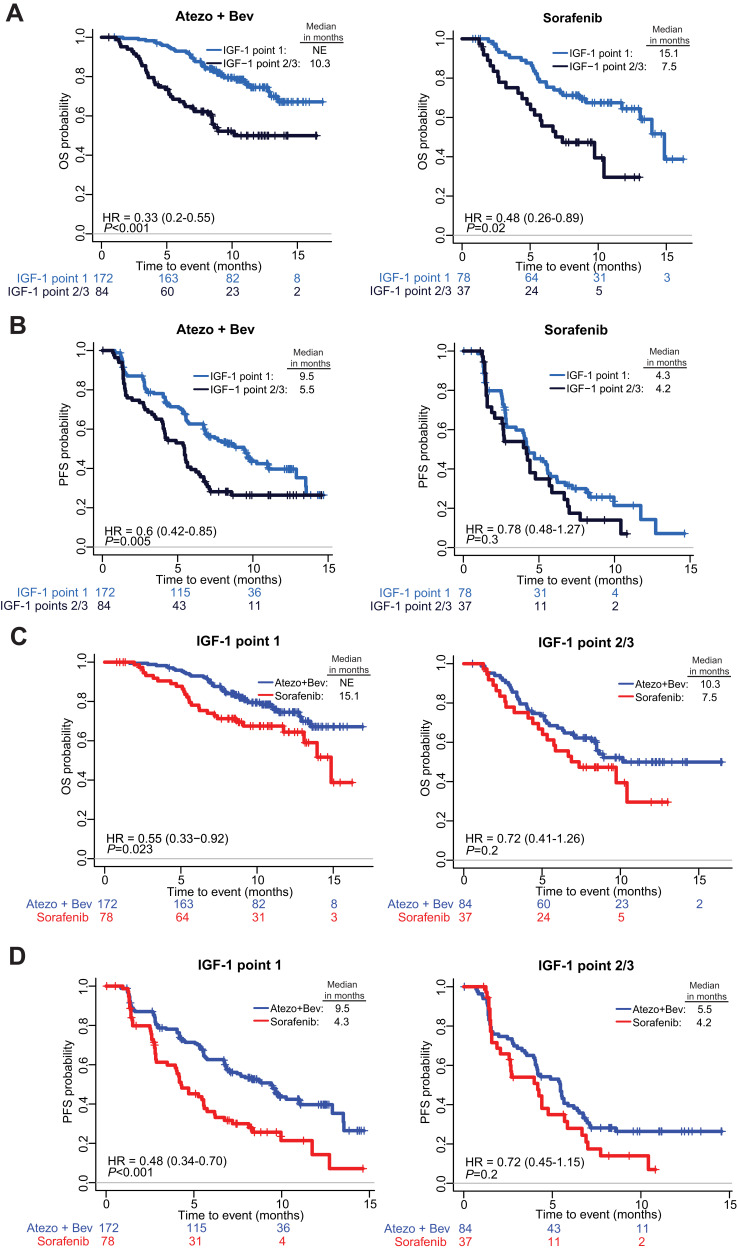
Baseline IGF-CTP score (A vs B/C) showed prognostic significance for OS in both the atezolizumab-bevacizumab (hazard ratio [HR], 0.33; 95% confidence interval [CI], 0.20-0.56; <0.001) and sorafenib (HR, 0.32; 95% CI, 0.16-0.65; =0.002) arms. Baseline IGF-1 score (1 vs 2/3) also showed prognostic significance for OS in both the atezolizumab-bevacizumab (HR, 0.33; 95% CI, 0.20-0.55; <0.001) and sorafenib (HR, 0.48; 95% CI, 0.26-0.89; =0.02) arms. HRs for PFS were consistent with those for OS. No significant predictive effects were observed for either score between the two arms. Kinetic analysis revealed that patients with increased IGF-1 score (1-> 2/3) at 3 weeks post treatment had shorter OS than patients with stable IGF-1 score of 1 in both the atezolizumab-bevacizumab (HR, 3.70; 95% CI, 1.56-8.77; =0.003) and sorafenib (HR, 5.83; 95% CI, 1.88-18.12; =0.0023) arms.
Baseline and kinetic change of IGF-CTP and IGF-1 scores are independent prognostic factors for patients with unresectable HCC treated with atezolizumab-bevacizumab or sorafenib. These novel scores may provide improved patient stratification in future HCC clinical trials. IMbrave150 ClincialTrials.gov number, NCT03434379.
Child-Turcotte-Pugh A类(CTP-A)用于不可切除肝细胞癌(HCC)是积极治疗和临床试验入组的标准标准。我们假设胰岛素样生长因子-1(IGF-1)衍生评分可能比CTP分类提供更好的生存预测。本研究旨在评估IGF-1衍生评分在III期IMbrave150研究中的潜在预后和预测作用。
对371例患者的基线和治疗期间血清IGF-1水平进行中心分析。根据预先设定的临界值确定患者的IGF-1评分(1/2/3)和IGF-CTP评分(A/B/C)。通过基线以及两个治疗组内和组间IGF-1和IGF-CTP评分的治疗期间变化分析结果。使用单因素和多因素分析评估这些评分与结果之间的相互作用。
基线IGF-CTP评分(A与B/C)在阿替利珠单抗-贝伐单抗(风险比[HR],0.33;95%置信区间[CI],0.20-0.56;<0.001)和索拉非尼(HR,0.32;95%CI,0.16-0.65;=0.002)组中对总生存期均显示出预后意义。基线IGF-1评分(1与2/3)在阿替利珠单抗-贝伐单抗(HR,0.33;95%CI,0.20-0.55;<0.001)和索拉非尼(HR,0.48;95%CI,0.26-0.89;=0.02)组中对总生存期也显示出预后意义。无进展生存期的HR与总生存期的HR一致。两组间任一评分均未观察到显著的预测作用。动态分析显示,在阿替利珠单抗-贝伐单抗(HR,3.70;95%CI,1.56-8.77;=0.003)和索拉非尼(HR,5.83;95%CI,1.88-18.12;=0.0023)组中,治疗后3周时IGF-1评分升高(1->2/3)的患者总生存期短于IGF-1评分为1且稳定的患者。
IGF-CTP和IGF-1评分的基线和动态变化是接受阿替利珠单抗-贝伐单抗或索拉非尼治疗的不可切除HCC患者的独立预后因素。这些新评分可能在未来的HCC临床试验中提供更好的患者分层。IMbrave150 美国国立医学图书馆临床试验注册中心编号,NCT03434379。