Lacin Sahin, Yalcin Suayib, Karakas Yusuf, Hassan Manal M, Amin Hesham, Mohamed Yehia Ibrahim, Rashid Asif, Morris Jeffrey S, Xiao Lianchun, Qayyum Aliya, Kaseb Ahmed O
Yeditepe University, Faculty of Medicine, Department of Medical Oncology, İstanbul, Turkey.
Hacettepe University, Hacettepe Cancer Institute, Department of Medical Oncology, Ankara, Turkey.
J Hepatocell Carcinoma. 2020 Sep 16;7:143-153. doi: 10.2147/JHC.S258930. eCollection 2020.
The Child-Turcotte-Pugh score (CTP) is the most commonly used tool to assess hepatic reserve and predict survival in hepatocellular cancer (HCC). The CTP stratification accuracy has been questioned and attempts have been made to improve the objectivity of the system. Serum insulin-like growth factor-1 (IGF-1)-CTP has been proposed to improve CTP prognostic accuracy. We aimed to validate the IGF-CTP score in our patient population.
A total of 84 diagnosed HCC patients were enrolled prospectively. IGF-CTP scores in addition to CTP scores were calculated. C-index was used to compare the prognostic significance of the two scoring systems and overall survival (OS).
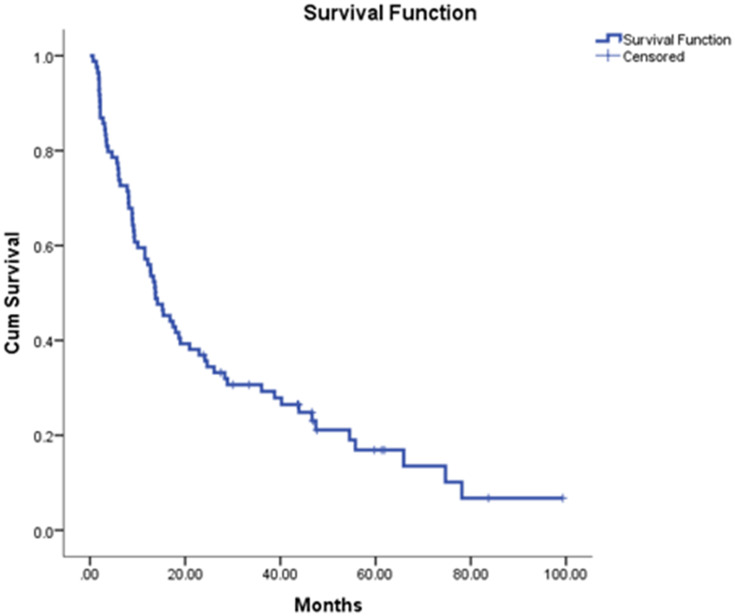
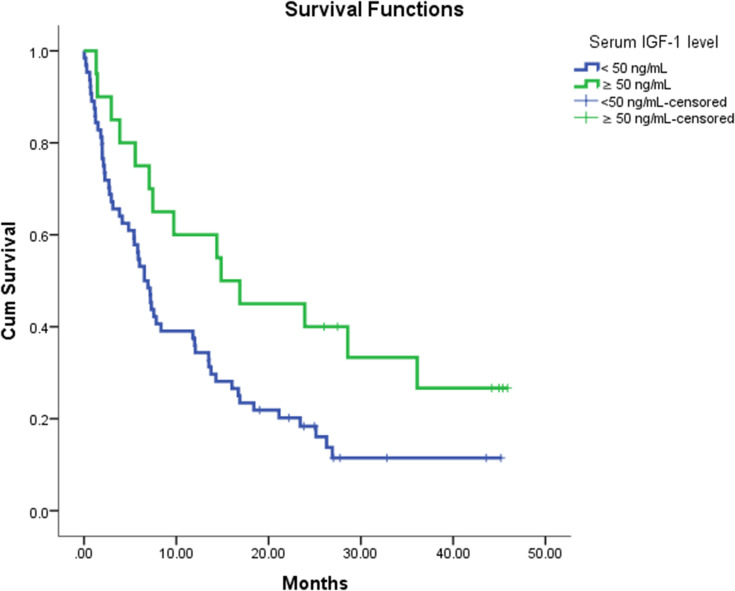
Cirrhosis was present in 48 (57.1%) patients, 35 (41.7%) patients were non-cirrhotic, 36 (42.8%) patients were hepatitis B (HBV) positive, and 8 (9.5%) patients were hepatitis C (HCV) positive. Serum IGF-1 levels were significantly lower in cirrhotic compared with non-cirrhotic patients (p=0.04). There was a significant difference in OS rates of patients with serum IGF-1 level <50 ng/mL and patients with serum IGF-1 levels ≥50 ng/mL (p=0.02); the OS rates were 6.5 and 14.8 months, respectively (p=0.02). The median OS of all patients was 7.38 months (95% CI: 5.89-13.79). The estimated C-index for CTP and IGF-CTP scores was 0.605 (95% CI: 0.538, 0.672) and 0.599 (95% CI: 0.543, 0.655), respectively. The U statistics indicated that the C-indices between two scoring systems are not statistically different (P= 0.91).
This study evaluated IGF-1 levels and the IGF-CTP classification in a predominantly HBV (+) cohort of HCC patients with 41.7% non-cirrhotic. Although the prognostic value was similar, among patients with CTP-A, class those reclassified as IGF-CTP B had shorter OS than those with IGF-CTP score A. Thus, further validations of IGF-CTP score in similar populations may add additional value as a stratification tool to predict HCC outcome.
Child-Turcotte-Pugh评分(CTP)是评估肝细胞癌(HCC)肝储备和预测生存情况最常用的工具。CTP分层的准确性受到质疑,人们已尝试提高该系统的客观性。血清胰岛素样生长因子-1(IGF-1)-CTP已被提出用于提高CTP的预后准确性。我们旨在验证IGF-CTP评分在我们患者群体中的有效性。
前瞻性纳入84例确诊的HCC患者。除CTP评分外,还计算了IGF-CTP评分。采用C指数比较两种评分系统的预后意义及总生存期(OS)。
48例(57.1%)患者存在肝硬化,35例(41.7%)患者无肝硬化,36例(42.8%)患者乙型肝炎(HBV)阳性,8例(9.5%)患者丙型肝炎(HCV)阳性。与无肝硬化患者相比,肝硬化患者的血清IGF-1水平显著降低(p = 0.04)。血清IGF-1水平<50 ng/mL的患者与血清IGF-1水平≥50 ng/mL的患者的OS率存在显著差异(p = 0.02);OS率分别为6.5个月和14.8个月(p = 0.02)。所有患者的中位OS为7.38个月(95%CI:5.89 - 13.79)。CTP和IGF-CTP评分的估计C指数分别为0.605(95%CI:0.538,0.672)和0.599(95%CI:0.543,0.655)。U统计量表明两种评分系统之间的C指数无统计学差异(P = 0.91)。
本研究在一个以HBV(+)为主、41.7%无肝硬化的HCC患者队列中评估了IGF-1水平及IGF-CTP分类。尽管预后价值相似,但在CTP-A级患者中,重新分类为IGF-CTP B级的患者的OS比IGF-CTP评分A级的患者短。因此,在类似人群中进一步验证IGF-CTP评分作为预测HCC预后的分层工具可能会增加额外价值。