Shirota Yuichiro, Otsuka Juuri, Toda Tatsushi, Hamada Masashi
Department of Neurology, Graduate School of Medicine, The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan.
Department of Clinical Laboratory, The University of Tokyo Hospital, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan.
Clin Neurophysiol Pract. 2022 Sep 23;7:273-278. doi: 10.1016/j.cnp.2022.09.002. eCollection 2022.
Using transcranial magnetic stimulation (TMS) to delineate upper motor neuron (UMN) signs of two neurodegenerative disorders: amyotrophic lateral sclerosis (ALS) and multiple system atrophy (MSA).
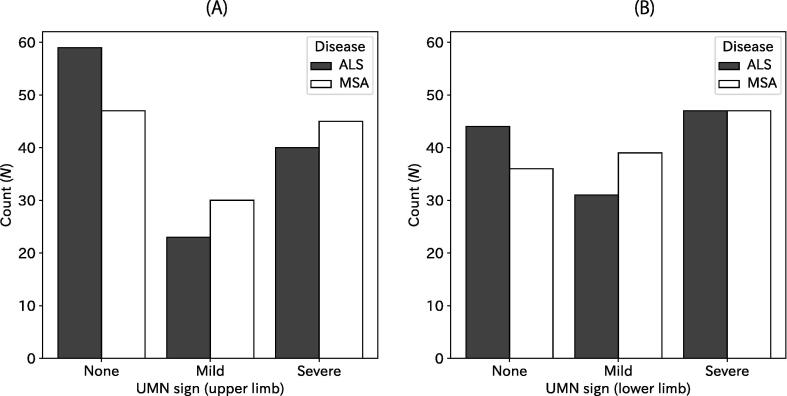
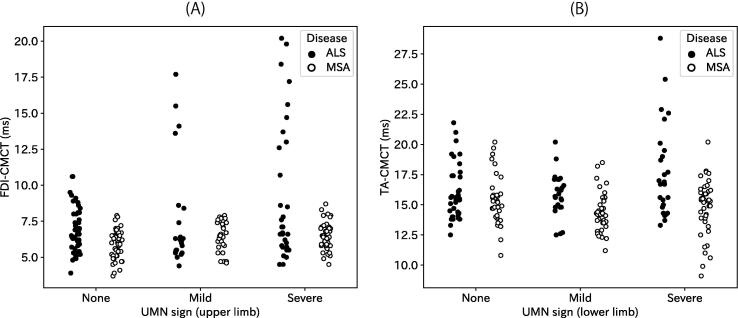
Medical records including clinical signs for UMN damage and TMS results were reviewed retrospectively. The UMN signs were classified into none, mild, and severe based on neurological examination of various reflexes. Then TMS-elicited motor evoked potentials (MEPs) were recorded from a hand and a leg muscle to calculate the central motor conduction time (CMCT), which represents fast, mono-synaptic conduction along the corticospinal tract. Relations between the UMN signs and CMCT were analysed for the two diseases.
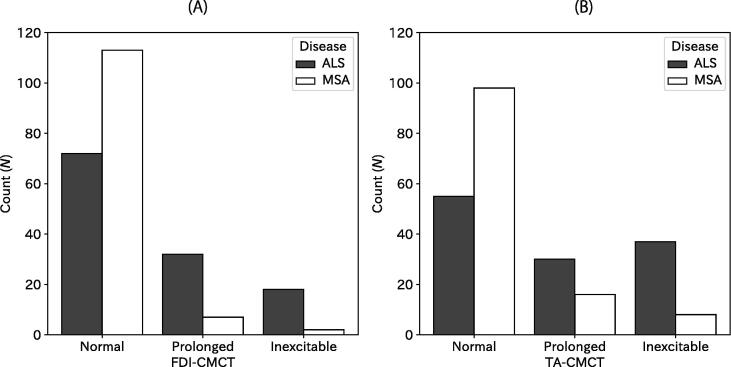
Prevalence and severity of the UMN signs for ALS and MSA were comparable for both upper and lower limbs. However, abnormality in CMCT was found more frequently in ALS: CMCT abnormalities were found in upper limbs for 44% in ALS patients but only for 7% in MSA patients; CMCT abnormalities in lower limbs were 55% in ALS and 20% in MSA. Some ALS patients showed abnormal CMCT in limbs without UMN signs, which was not true for most MSA patients.
The abnormalities of CMCT were different in ALS and MSA, even for those who clinically had similar UMN signs. Sometimes, CMCT can reveal UMN damage in the absence of clinical UMN signs. Differences presumably derive from selective degeneration of different fibres in the motor descending pathways. Longitudinal studies must be conducted to accumulate neuroimaging and pathological findings.
CMCT can be useful to differentiate ALS and MSA.
运用经颅磁刺激(TMS)描绘两种神经退行性疾病——肌萎缩侧索硬化症(ALS)和多系统萎缩症(MSA)的上运动神经元(UMN)体征。
回顾性分析包含UMN损伤临床体征及TMS结果的病历。基于对各种反射的神经学检查,将UMN体征分为无、轻度和重度。然后从手部和腿部肌肉记录TMS诱发的运动诱发电位(MEP),以计算中枢运动传导时间(CMCT),其代表沿皮质脊髓束的快速单突触传导。分析这两种疾病中UMN体征与CMCT之间的关系。
ALS和MSA的UMN体征在上肢和下肢的患病率及严重程度相当。然而,CMCT异常在ALS中更为常见:ALS患者上肢CMCT异常的比例为44%,而MSA患者仅为7%;ALS患者下肢CMCT异常的比例为55%,MSA患者为20%。一些ALS患者在无UMN体征的肢体中显示CMCT异常,而大多数MSA患者并非如此。
即使对于临床UMN体征相似的患者,ALS和MSA的CMCT异常情况也有所不同。有时,CMCT可在无临床UMN体征时揭示UMN损伤。差异可能源于运动下行通路中不同纤维的选择性退化。必须开展纵向研究以积累神经影像学和病理学发现。
CMCT有助于鉴别ALS和MSA。