VA Boston Cooperative Studies Program, Boston, Massachusetts.
VA Palo Alto Healthcare System, Palo Alto, California.
JAMA Netw Open. 2022 Oct 3;5(10):e2240037. doi: 10.1001/jamanetworkopen.2022.40037.
With a large proportion of the US adult population vaccinated against SARS-CoV-2, it is important to identify who remains at risk of severe infection despite vaccination.
To characterize risk factors for severe COVID-19 disease in a vaccinated population.
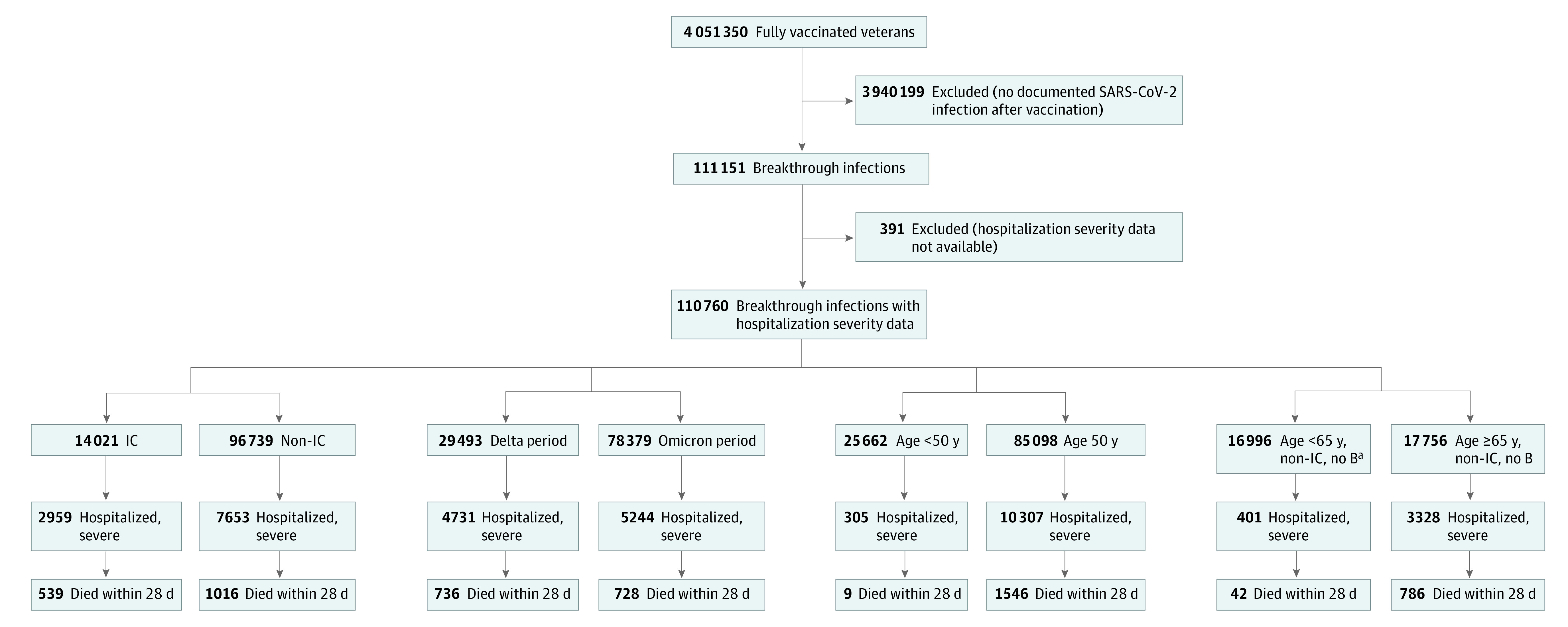
DESIGN, SETTING, AND PARTICIPANTS: This nationwide, retrospective cohort study included US veterans who received a SARS-CoV-2 vaccination series and later developed laboratory-confirmed SARS-CoV-2 infection and were treated at US Department of Veterans Affairs (VA) hospitals. Data were collected from December 15, 2020, through February 28, 2022.
Demographic characteristics, comorbidities, immunocompromised status, and vaccination-related variables.
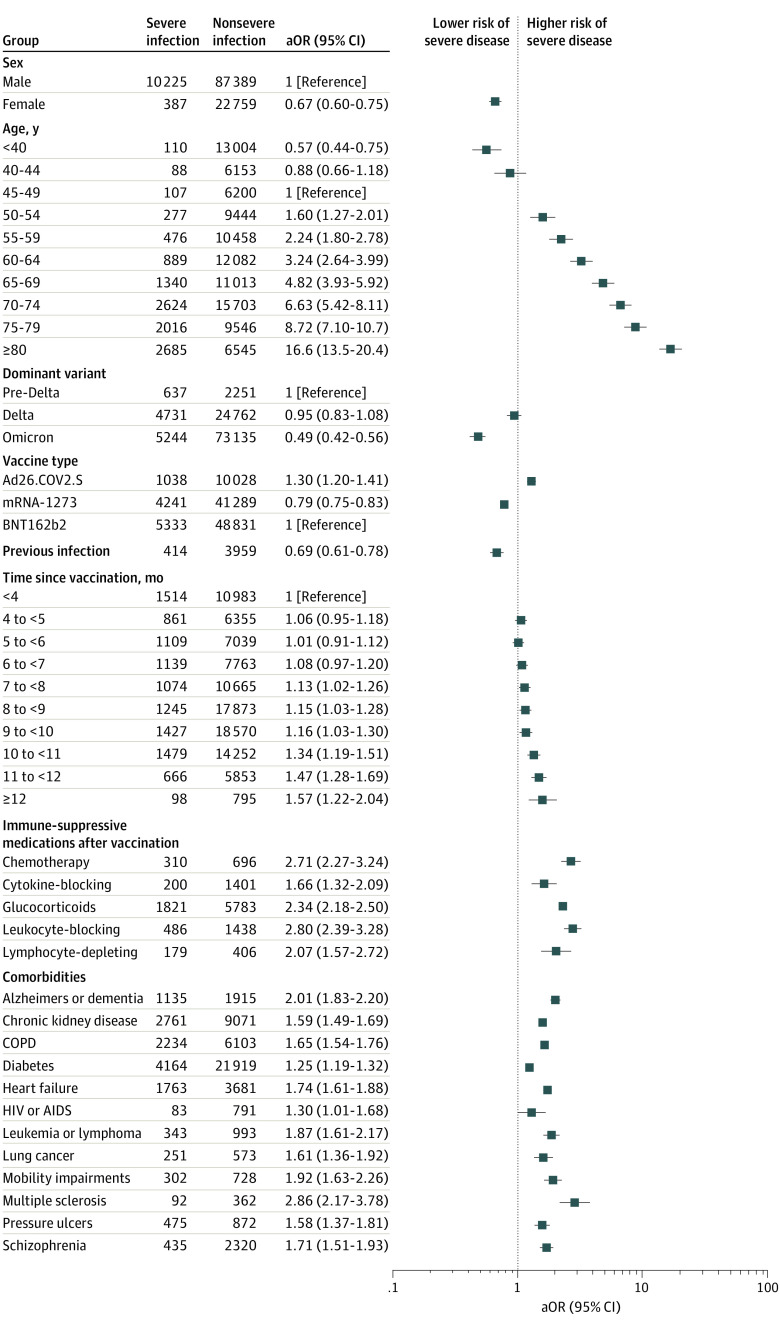
Development of severe vs nonsevere SARS-CoV-2 infection. Severe disease was defined as hospitalization within 14 days of a positive SARS-CoV-2 diagnostic test and either blood oxygen level of less than 94%, receipt of supplemental oxygen or dexamethasone, mechanical ventilation, or death within 28 days. Association between severe disease and exposures was estimated using logistic regression models.
Among 110 760 patients with infections following vaccination (97 614 [88.1%] men, mean [SD] age at vaccination, 60.8 [15.3] years; 26 953 [24.3%] Black, 11 259 [10.2%] Hispanic, and 71 665 [64.7%] White), 10 612 (9.6%) had severe COVID-19. The strongest association with risk of severe disease after vaccination was age, which increased among patients aged 50 years or older with an adjusted odds ratio (aOR) of 1.42 (CI, 1.40-1.44) per 5-year increase in age, such that patients aged 80 years or older had an aOR of 16.58 (CI, 13.49-20.37) relative to patients aged 45 to 50 years. Immunocompromising conditions, including receipt of different classes of immunosuppressive medications (eg, leukocyte inhibitor: aOR, 2.80; 95% CI, 2.39-3.28) or cytotoxic chemotherapy (aOR, 2.71; CI, 2.27-3.24) prior to breakthrough infection, or leukemias or lymphomas (aOR, 1.87; CI, 1.61-2.17) and chronic conditions associated with end-organ disease, such as heart failure (aOR, 1.74; CI, 1.61-1.88), dementia (aOR, 2.01; CI, 1.83-2.20), and chronic kidney disease (aOR, 1.59; CI, 1.49-1.69), were also associated with increased risk. Receipt of an additional (ie, booster) dose of vaccine was associated with reduced odds of severe disease (aOR, 0.50; CI, 0.44-0.57).
In this nationwide, retrospective cohort of predominantly male US Veterans, we identified risk factors associated with severe disease despite vaccination. Findings could be used to inform outreach efforts for booster vaccinations and to inform clinical decision-making about patients most likely to benefit from preexposure prophylaxis and antiviral therapy.
由于美国很大一部分成年人接种了 SARS-CoV-2 疫苗,因此确定尽管接种了疫苗但仍有感染严重感染风险的人群是很重要的。
描述接种疫苗人群中 COVID-19 严重疾病的危险因素。
设计、地点和参与者:这项全国性的回顾性队列研究包括在美国退伍军人事务部(VA)医院接受 SARS-CoV-2 疫苗接种系列接种后发生实验室确诊 SARS-CoV-2 感染并接受治疗的美国退伍军人。数据收集时间为 2020 年 12 月 15 日至 2022 年 2 月 28 日。
人口统计学特征、合并症、免疫功能低下状态和疫苗接种相关变量。
发展为严重与非严重 SARS-CoV-2 感染。严重疾病定义为在 SARS-CoV-2 诊断性检测呈阳性后 14 天内住院,并且血氧水平低于 94%,接受补充氧气或地塞米松、机械通气或 28 天内死亡。使用逻辑回归模型估计严重疾病与暴露之间的关联。
在接种疫苗后发生感染的 110760 例患者中(97614 [88.1%] 为男性,接种疫苗时的平均[SD]年龄为 60.8 [15.3] 岁;26953 [24.3%] 为黑人,11259 [10.2%] 为西班牙裔,71665 [64.7%] 为白人),10612 例(9.6%)患有严重 COVID-19。与接种疫苗后发生严重疾病风险最强相关的是年龄,50 岁或以上的患者每增加 5 岁,调整后的优势比(aOR)增加 1.42(CI,1.40-1.44),例如 80 岁或以上的患者的 aOR 为 16.58(CI,13.49-20.37)与 45 至 50 岁的患者相比。免疫功能低下的情况,包括接受不同类别的免疫抑制药物(例如白细胞抑制剂:aOR,2.80;95%CI,2.39-3.28)或细胞毒性化疗(aOR,2.71;CI,2.27-3.24),或白血病或淋巴瘤(aOR,1.87;CI,1.61-2.17)和与终末器官疾病相关的慢性疾病,如心力衰竭(aOR,1.74;CI,1.61-1.88)、痴呆症(aOR,2.01;CI,1.83-2.20)和慢性肾病(aOR,1.59;CI,1.49-1.69),也与增加的风险相关。接种额外(即加强)剂量的疫苗与严重疾病的几率降低相关(aOR,0.50;CI,0.44-0.57)。
在这项针对美国退伍军人的全国性回顾性队列研究中,我们确定了尽管接种了疫苗但仍存在严重疾病的危险因素。研究结果可用于为加强疫苗接种提供信息,并为最有可能从暴露前预防和抗病毒治疗中获益的患者的临床决策提供信息。